อ่าน 23 นาที
Tracheotomy
Tracheotomy (/ˌtreɪkiˈɒtəmi/, UK also/ˌtræki-/), or tracheostomy, is a surgical airway management procedure which consists of making an incision on the front of the neck to open a.
Tracheotomy
| Tracheotomy | |
|---|---|
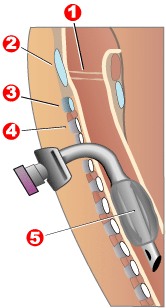 Completed tracheotomy: 1 – Vocal folds 2 – Thyroid cartilage 3 – Cricoid cartilage 4 – Tracheal rings 5 – Balloon cuff | |
| ICD-10-PCS | 0B110F4 |
| ICD-9-CM | 31.1 |
| MeSH | D014140 |
| MedlinePlus | 002955 |
Tracheotomy (/ˌtreɪkiˈɒtəmi/, UK also/ˌtræki-/), or tracheostomy, is a surgical airway management procedure which consists of making an incision on the front of the neck to open a direct airway to the trachea. The resulting stoma (hole) can serve independently as an airway or as a site for a tracheal tube (or tracheostomy tube) to be inserted;[1] this tube allows a person to breathe without the use of the nose or mouth.
Etymology and terminology

The etymology of the word tracheotomy comes from two Greek words: the roottom- (from Greek τομή tomḗ) meaning "to cut", and the word trachea (from Greek τραχεία tracheía).[2] The word tracheostomy, including the root stom- (from Greek στόμα stóma) meaning "mouth", refers to the making of a semi-permanent or permanent opening and to the opening itself. Some sources offer different definitions of the above terms. Part of the ambiguity is due to the uncertainty of the intended permanence of the stoma (hole) at the time it is created.[3]
Indications
There are four main reasons why someone would receive a tracheotomy:[3]
- Emergency airway access
- Airway access for prolonged mechanical ventilation
- Functional or mechanical upper airway obstruction
- Decreased/incompetent clearance of tracheobronchial secretions
In the acute (short term) setting, indications for tracheotomy include such conditions as severe facial trauma, tumors of the head and neck (e.g., cancers, branchial cleft cysts), and acute angioedema (swelling) and inflammation of the head and neck. In the context of failed tracheal intubation, either tracheotomy or cricothyrotomy may be performed.

In the chronic (long-term) setting, indications for tracheotomy include the need for long-term mechanical ventilation and tracheal toilet (e.g., comatose patients, extensive surgery involving the head and neck). Tracheotomy may result in a significant reduction in the administration of sedatives and vasopressors, as well as the duration of stay in the intensive care unit (ICU).[4]
In extreme cases, the procedure may be indicated as a treatment for severe obstructive sleep apnea (OSA) seen in patients intolerant of continuous positive airway pressure (CPAP) therapy. The reason tracheostomy works well for OSA is that it is the only surgical procedure that completely bypasses the upper airway. This procedure was commonly performed for obstructive sleep apnea until the 1980s, when other procedures such as the uvulopalatopharyngoplasty, genioglossus advancement, and maxillomandibular advancement surgeries were described as alternative surgical modalities for OSA.
If prolonged ventilation is required, tracheostomy is usually considered. The timing of this procedure is dependent on the clinical situation and an individual's preference. An international multicenter study in 2000 determined that the median time between starting mechanical ventilation and receiving a tracheostomy was 11 days.[5] Although the definition varies depending on hospital and provider, early tracheostomy can be considered to be less than 10 days (2 to 14 days) and late tracheostomy to be 10 days or more.
Alternatives
Biphasic cuirass ventilation is a form of non-invasive mechanical ventilation that can — in a small subset of cases — allow people to avoid a tracheostomy.[6]
Components

A tracheostomy tube may be single or dual lumen, and also cuffed or uncuffed. A dual lumen tracheostomy tube consists of an outer cannula or main shaft, an inner cannula, and an obturator. The obturator is used when inserting the tracheostomy tube to guide the placement of the outer cannula and is removed once the outer cannula is in place. The outer cannula remains in place but, because of the buildup of secretions, there is an inner cannula that may be removed for cleaning after use or it may be replaced. Single-lumen tracheostomy tubes do not have a removable inner cannula, suitable for narrower airways. Cuffed tracheostomy tubes have inflatable balloons at the end of the tube to secure them in place. A tracheostomy tube may be fenestrated with one or several holes to let air through the larynx, allowing speech.[7]
Special tracheostomy tube valves (such as the Passy-Muir valve[8]) have been created to assist people in their speech. The patient can inhale through the unidirectional tube. Upon expiration, pressure causes the valve to close, redirecting air around the tube, past the vocal folds, producing sound.[9]
Surgical procedure
Open surgical tracheotomy (OST)
The typical procedure done is the open surgical tracheotomy (OST) and is usually done in a sterile operating room. The optimal patient position involves a cushion under the shoulders to extend the neck. Commonly a transverse (horizontal) incision is made two fingerbreadths above the suprasternal notch. Alternatively, a vertical incision can be made in the midline of the neck from the thyroid cartilage to just above the suprasternal notch. Skin, subcutaneous tissue, and strap muscles (a specific group of neck muscles) are retracted aside to expose the thyroid isthmus, which can be cut or retracted upwards. After proper identification of the cricoid cartilage and placement of a tracheal hook to steady the trachea and pull it forward, the trachea is cut open, either through the space between cartilage rings or vertically across multiple rings (cruciate incision). Occasionally a section of a tracheal cartilage ring may be removed to make insertion of the tube easier. Once the incision is made, a properly sized tube is inserted. The tube is connected to a ventilator and adequate ventilation and oxygenation is confirmed. The tracheotomy apparatus is then attached to the neck with tracheotomy ties, skin sutures, or both.[10][11]
Percutaneous dilatational tracheotomy (PDT)
The first widely accepted percutaneous tracheotomy technique was described by Pat Ciaglia, a New York surgeon, in 1985.[12] The next widely used technique was developed in 1989 by Bill Griggs, an Australian intensive care specialist.[13] In 1995, Fantoni developed a translaryngeal approach of percutaneous tracheostomy.[14] The Griggs and Ciaglia Blue Rhino techniques are the two main techniques in current use. A number of comparison studies have been undertaken between these two techniques with no clear differences emerging.[15] An advantage of PDT over OST is the ability to perform the procedure at the patient's bedside. This significantly decreases costs and time/people-power needed for an operating room (OR) procedure.[11] Contraindications for percutaneous tracheostomy include infection at the site of tracheostomy, uncontrolled bleeding disorder, unstable cardiopulmonary status, patient unable to stay still, abnormal anatomy of the tracheolaryngeal structures.[2]
Risks and complications
As with most other surgical procedures, some cases are more difficult than others. Surgery on children is more difficult because of their smaller size. Difficulties such as a short neck and bigger thyroid glands make the trachea hard to open.[16] There are other difficulties with patients with irregular necks, the obese, and those with a large goitre.
The many possible complications include hemorrhage, loss of airway, subcutaneous emphysema, wound infections, stoma cellulites, fracture of tracheal rings, poor placement of the tracheostomy tube, and bronchospasm.[17]
Early complications include infection, hemorrhage, pneumomediastinum, pneumothorax, tracheoesophageal fistula, recurrent laryngeal nerve injury, and tube displacement. Delayed complications include tracheal-innominate artery fistula, tracheal stenosis, delayed tracheoesophageal fistula, and tracheocutaneous fistula.[10]
A 2013 systematic review (published cases from 1985 to April 2013) studied the complications and risk factors of percutaneous dilatational tracheostomy (PDT), identifying major causes of fatality to be hemorrhage (38.0%), airway complications (29.6%), tracheal perforation (15.5%), and pneumothorax (5.6%)[18] A similar systematic review in 2017 (cases from 1990 to 2015) studying fatality in both open surgical tracheotomy (OST) and PDT identified similar rates of mortality and causes of death between the two techniques.[19]
Hemorrhage is rare, but the most likely cause of fatality after a tracheostomy. It usually occurs due to a tracheoarterial fistula, an abnormal connection between the trachea and nearby blood vessels, and most commonly manifests between 3 days to 6 weeks after the procedure is done. Fistulas can result from incorrectly positioned equipment, high cuff pressures causing pressure sores or mucosal damage, a low surgical trachea site, repetitive neck movement, radiotherapy, or prolonged intubation.[20]
A potential risk factor identified in a 2013 systematic review of the percutaneous technique was the lack of bronchoscopic guidance. Use of the bronchoscope, an instrument inserted through a patient's mouth for internal visualization of the airway, can help with proper placement of instruments and better visualization of anatomical structures. However, this can also be dependent on the skills and familiarity of the surgeon with both the procedure and the patient's anatomy.[18]
There are a multitude of potential complications related to the airway. The main causes of mortality during PDT include dislodgment of the tube, loss of airway during procedure and misplacement of the tube.[18] One of the more urgent complications include displacement or dislodgment of the tracheotomy tube, either spontaneously or during a tube change. Although uncommon (< 1/1000 tracheostomy tube days), the associated fatality is high due to the loss of airway.[21] Due to the seriousness of such a situation, individuals with a tracheotomy tube should consult with their healthcare providers to have a specific, written, emergency intubation and tracheostomy recannulation (reinsertion) plan prepared in advance.
Tracheal stenosis, otherwise known as an abnormal narrowing of the airway, is a possible long term complication. The most common symptom of stenosis is gradually-worsening difficulty with breathing (dyspnea). However incidence is low, ranging from 0.6 to 2.8% with increased rates if major bleeding or wound infections are present. A 2016 systematic review identified a higher rate of tracheal stenosis in individuals who underwent a surgical tracheostomy, as compared to PDT, however the difference was not statistically significant.[22]
A 2000 Spanish study of bedside percutaneous tracheostomy reported overall complication rates of 10–15% and a procedural mortality of 0%,[23] which is comparable to those of other series reported in the literature from the Netherlands[24][25] and the United States.[26][27] A 2013 systematic review calculated procedural mortality to be 0.17% or 1 in 600 cases.[18] Multiple systematic reviews identified no significant difference in rates of mortality, major bleeding, or wound infection between the percutaneous or open surgical methods.[22][19]
Specifically a 2017 systematic review calculated the most common causes of death and their frequencies, out of all tracheotomies, to be hemorrhage (OST: 0.26%, PDT: 0.19%), loss of airway (OST: 0.21%, PDT: 0.20%), and misplacement of tube (OST: 0.11%, PDT: 0.20%).[19]
A 2003 American cadaveric study identified multiple tracheal ring fractures with the Ciaglia Blue Rhino technique as a complication occurring in 100% of their small series of cases.[28] The comparative study above also identified ring fractures in 9 of 30 live patients[15] while another small series identified ring fractures in 5 of their 20 patients.[29] The long term significance of tracheal ring fractures is unknown.[30]
History

Ancient history
Tracheotomy was first potentially depicted on Egyptian artifacts in 3600 BC.[31]Hippocrates condemned the practice of tracheotomy as incurring an unacceptable risk of damage to the carotid artery. Warning against the possibility of death from inadvertent laceration of the carotid artery during tracheotomy, he instead advocated the practice of tracheal intubation.[17]
Despite the concerns of Hippocrates, it is believed that an early tracheotomy was performed by Asclepiades of Bithynia, who lived in Rome around 100 BC.[32]Galen and Aretaeus, both of whom lived in Rome in the 2nd century AD, credit Asclepiades as being the first physician to perform a non-emergency tracheotomy. Antyllus, another Roman-era Greek physician of the 2nd century AD, supported tracheotomy when treating oral diseases. He refined the technique to be more similar to that used in modern times, recommending that a transverse incision be made between the third and fourth tracheal rings for the treatment of life-threatening airway obstruction.[17]
Medieval world
The 7th century Byzantine physician Paul of Aegina, an advocate of the procedure, acknowledged previous Greek authors' works on the subject of tracheotomies and provided descriptions of the procedure in his own works.[33] In 1000, Abu al-Qasim al-Zahrawi (936–1013), an Arab who lived in Arabic Spain, published the 30-volume Kitab al-Tasrif, the first illustrated work on surgery. He never performed a tracheotomy, but he did treat a slave girl who had cut her own throat in a suicide attempt. Al-Zahrawi (known to Europeans as Albucasis) sewed up the wound and the girl recovered, thereby proving that an incision in the larynx could heal. Circa AD 1020, Avicenna (980–1037) described tracheal intubation in The Canon of Medicine in order to facilitate breathing.[34] The first clear description of the tracheotomy operation for treating asphyxiation was given by Ibn Zuhr (1091–1161) in the 12th century. According to Mostafa Shehata, Ibn Zuhr (also known as Avenzoar) successfully practiced the tracheotomy procedure on a goat, justifying Galen's approval of the operation.[35]
16th–18th centuries

ยุคฟื้นฟูศิลปวิทยาการของยุโรปนำมาซึ่งความก้าวหน้าอย่างมากในทุกสาขาวิทยาศาสตร์ โดยเฉพาะอย่างยิ่งการผ่าตัด ความรู้ด้านกายวิภาคที่เพิ่มขึ้นเป็นปัจจัยสำคัญในการพัฒนาเหล่านี้ ศัลยแพทย์เปิดรับการผ่าตัดทดลองบนหลอดลมมากขึ้น ในช่วงเวลานี้ ศัลยแพทย์หลายคนพยายามทำการเจาะหลอดลมด้วยเหตุผลต่างๆ และด้วยวิธีการต่างๆ มีข้อเสนอแนะมากมาย แต่ความคืบหน้าที่แท้จริงในการทำให้ขั้นตอนประสบความสำเร็จมากขึ้นนั้นมีน้อยมาก การเจาะหลอดลมยังคงเป็นการผ่าตัดที่อันตรายและมีอัตราความสำเร็จต่ำมาก และศัลยแพทย์หลายคนยังคงพิจารณาว่าการเจาะหลอดลมเป็นขั้นตอนที่ไร้ประโยชน์และอันตราย อัตราการเสียชีวิตที่สูงจากการผ่าตัดนี้ ซึ่งไม่ได้ดีขึ้นเลย สนับสนุนจุดยืนของพวกเขา ตั้งแต่ปี ค.ศ. 1500 ถึง 1832 มีรายงานการเจาะหลอดลมที่รู้จักเพียง 28 รายงานเท่านั้น[ 36 ]
ในปี ค.ศ. 1543 Andreas Vesalius (1514–1564) เขียนว่าการใส่ท่อช่วยหายใจและการช่วยหายใจเทียม ในภายหลัง สามารถช่วยชีวิตได้Antonio Musa Brassavola (1490–1554) แห่งเมืองเฟอร์รารารักษาผู้ป่วยที่มีฝีรอบต่อมทอนซิล ด้วยการเจาะหลอดลมหลังจากที่ ศัลยแพทย์ช่างตัดผมปฏิเสธการรักษา ผู้ป่วยดูเหมือนจะหายเป็นปกติ และ Brassavola ได้ตีพิมพ์บันทึกของเขาในปี ค.ศ. 1546 การผ่าตัดนี้ได้รับการระบุว่าเป็นการเจาะหลอดลมที่ประสบความสำเร็จครั้งแรกที่มีการบันทึกไว้ แม้ว่าจะมีการอ้างอิงถึงหลอดลมและอาจรวมถึงการเปิดหลอดลมในสมัยโบราณมากมายก็ตาม[ 36 ] Ambroise Paré (1510–1590) อธิบายถึงการเย็บแผลฉีกขาดของหลอดลมในช่วงกลางศตวรรษที่ 16 ผู้ป่วยรายหนึ่งรอดชีวิตแม้จะมีอาการบาดเจ็บที่หลอดเลือดดำภายในคอร่วมด้วย อีกรายหนึ่งได้รับบาดเจ็บที่หลอดลมและหลอดอาหารและเสียชีวิต
ในช่วงปลายศตวรรษที่ 16 นักกายวิภาคศาสตร์และศัลยแพทย์ฮีโรนีมัส ฟาบริซิอุส (ค.ศ. 1533–1619) ได้อธิบายเทคนิคการเจาะหลอดลมที่มีประโยชน์ในงานเขียนของเขา แม้ว่าเขาจะไม่เคยทำการผ่าตัดด้วยตนเองก็ตาม เขาแนะนำให้ใช้การผ่าตัดแนวตั้ง และเป็นคนแรกที่นำเสนอแนวคิดเรื่องท่อเจาะหลอดลม ท่อนี้เป็นท่อ สั้นตรง ที่มีปีกเพื่อป้องกันไม่ให้ท่อเข้าไปในหลอดลมมากเกินไป เขาแนะนำให้ทำการผ่าตัดนี้เป็นทางเลือกสุดท้ายเท่านั้น ในกรณีที่ทางเดินหายใจอุดตันจากสิ่งแปลกปลอมหรือสารคัดหลั่งคำอธิบายขั้นตอนการเจาะหลอดลมของฟาบริซิอุสคล้ายคลึงกับที่ใช้ในปัจจุบันจูลิโอ เซซาเร คาสเซรี (ค.ศ. 1552–1616) สืบทอดตำแหน่งศาสตราจารย์ด้านกายวิภาคศาสตร์ที่มหาวิทยาลัยปาดัวต่อจากฟาบริซิอุส และตีพิมพ์งานเขียนของตนเองเกี่ยวกับเทคนิคและอุปกรณ์สำหรับการเจาะหลอดลม คาสเซรีแนะนำให้ใช้ท่อเงินโค้งที่มีรูหลายรูมาร์โก ออเรลิโอ เซเวริโน (1580–1656) ศัลยแพทย์และนักกายวิภาคศาสตร์ผู้เชี่ยวชาญ ได้ทำการผ่าตัดหลอดลมสำเร็จหลายครั้งในช่วงการระบาดของ โรค คอตีบ ในเนเปิลส์ในปี 1610 โดยใช้เทคนิคการผ่าตัดแนวตั้งที่ฟาบริเซียสแนะนำ นอกจากนี้เขายังพัฒนาเครื่องมือเจาะหลอดลมแบบฉบับของตนเองอีกด้วย[ 37 ]
ในปี ค.ศ. 1620 ศัลยแพทย์ชาวฝรั่งเศสนิโคลัส ฮาบิโคต์ (ค.ศ. 1550–1624) ศัลยแพทย์ของดยุคแห่งเนมูร์และนักกายวิภาคศาสตร์ ได้ตีพิมพ์รายงานเกี่ยวกับการผ่าตัดหลอดลมที่ประสบความสำเร็จ 4 ครั้งที่เขาได้ทำการผ่าตัด[ 38 ]หนึ่งในนั้นเป็นกรณีแรกที่บันทึกไว้ของการผ่าตัดหลอดลมเพื่อเอาสิ่งแปลกปลอมออก ในกรณีนี้คือลิ่มเลือดในกล่องเสียงของผู้ที่ถูกแทง เขายังได้อธิบายถึงการผ่าตัดหลอดลมครั้งแรกที่ทำกับ ผู้ป่วย เด็กเด็กชายอายุ 14 ปีกลืนถุงที่บรรจุเหรียญทอง 9 เหรียญเข้าไปเพื่อพยายามป้องกันการถูกขโมยโดยโจร บน ทางหลวงวัตถุนั้นติดอยู่ในหลอดอาหาร ของเขา ขัดขวางหลอดลม ฮาบิโคต์แนะนำว่าการผ่าตัดนี้อาจได้ผลกับผู้ป่วยที่มีอาการอักเสบของกล่องเสียงด้วย เขาได้พัฒนาอุปกรณ์สำหรับการผ่าตัดนี้ซึ่งมีความคล้ายคลึงกับการออกแบบในปัจจุบัน (ยกเว้นการใช้ท่อเดี่ยวของเขา)
เชื่อกันว่า Sanctorius (1561–1636) เป็นคนแรกที่ใช้ trocar ในการผ่าตัด และเขาแนะนำให้ทิ้ง cannula ไว้ในตำแหน่งเดิมเป็นเวลาสองสามวันหลังการผ่าตัด[ 39 ]อุปกรณ์เจาะหลอดลมในยุคแรกๆ มีภาพประกอบอยู่ในQuestion Chirurgicale ของ Habicot [ 38 ] และ Tabulae anatomicaeที่ตีพิมพ์หลังมรณกรรมของ Casseri ในปี 1627 [ 40 ] Thomas Fienus (1567–1631) ศาสตราจารย์ด้านการแพทย์ที่มหาวิทยาลัย Louvainเป็นคนแรกที่ใช้คำว่า "tracheotomy" ในปี 1649 แต่คำนี้ไม่ได้ใช้กันอย่างแพร่หลายจนกระทั่งอีกหนึ่งศตวรรษต่อมา[ 41 ] Georg Detharding (1671–1747) ศาสตราจารย์ด้านกายวิภาคศาสตร์ที่มหาวิทยาลัย Rostockได้ทำการรักษาผู้ที่จมน้ำด้วยการเจาะหลอดลมในปี 1714 [ 42 ] [ 43 ] [ 44 ]
ศตวรรษที่ 19
ในช่วงทศวรรษ 1820 การเจาะหลอดลมเริ่มได้รับการยอมรับว่าเป็นวิธีการรักษาที่ถูกต้องสำหรับการอุดตันทางเดินหายใจอย่างรุนแรง ในปี 1832 แพทย์ชาวฝรั่งเศสPierre Bretonneau ได้ใช้การ เจาะ หลอดลม เป็นทางเลือกสุดท้ายในการรักษาโรคคอตีบ[ 45 ] ในปี 1852 Armand Trousseauนักศึกษาของ Bretonneau ได้รายงานการเจาะหลอดลมจำนวน 169 ครั้ง (158 ครั้งสำหรับ โรค ครูปและ 11 ครั้งสำหรับ "โรคเรื้อรังของกล่องเสียง") [ 46 ]ในปี 1858 John Snow เป็นคนแรกที่รายงานการเจาะหลอดลมและการใส่ท่อเข้าไปในหลอดลมเพื่อใช้ในการให้ยาสลบคลอโรฟอร์มในแบบจำลองสัตว์[ 47 ]ในปี พ.ศ. 2414 ศัลยแพทย์ชาวเยอรมันฟรีดริช เทรนเดเลนบูร์ก (พ.ศ. 2487–2467) ได้ตีพิมพ์บทความที่อธิบายถึงการผ่าตัดเจาะหลอดลมในมนุษย์ครั้งแรกที่ประสบความสำเร็จเพื่อจุดประสงค์ในการให้ยาสลบ[ 48 ]ในปี พ.ศ. 2423 ศัลยแพทย์ชาวสกอตแลนด์วิลเลียม แมคอีเวน (พ.ศ. 2491–2467) ได้รายงานเกี่ยวกับการใช้การใส่ท่อช่วยหายใจทางปากและหลอดลมเป็นทางเลือกแทนการเจาะหลอดลมเพื่อให้ผู้ป่วยที่มีอาการบวมของกล่องเสียงสามารถหายใจได้ เช่นเดียวกับการใช้ในบริบทของการดมยาสลบด้วยคลอโรฟอร์ม[ 49 ] [ 50 ] ในที่สุด ในปี พ.ศ. 2423 หนังสือของ โมเรลล์ แมคเคนซีได้กล่าวถึงอาการที่บ่งชี้ว่าจำเป็นต้องเจาะหลอดลมและเมื่อใดที่การผ่าตัดนั้นจำเป็นอย่างยิ่ง[ 17 ]
ศตวรรษที่ 20

ในช่วงต้นศตวรรษที่ 20 แพทย์เริ่มใช้การเจาะหลอดลมในการรักษาผู้ป่วยที่เป็นอัมพาตจากโรคโปลิโอที่ต้องใช้เครื่องช่วยหายใจอย่างไรก็ตาม ศัลยแพทย์ยังคงถกเถียงกันในแง่มุมต่างๆ ของการเจาะหลอดลมไปจนถึงศตวรรษที่ 20 มีการอธิบายและนำเทคนิคต่างๆ มาใช้มากมาย รวมถึงเครื่องมือผ่าตัดและท่อหลอดลมที่แตกต่างกัน ศัลยแพทย์ดูเหมือนจะไม่สามารถหาข้อสรุปได้ว่าควรทำการเจาะหลอดลมที่ใดหรืออย่างไร โดยถกเถียงกันว่า "การเจาะหลอดลมสูง" หรือ "การเจาะหลอดลมต่ำ" แบบไหนมีประโยชน์มากกว่ากัน เทคนิคการเจาะหลอดลมที่ใช้ในปัจจุบันได้รับการอธิบายไว้ในปี 1909 โดยเชวาลิเยร์ แจ็กสันแห่งเมืองพิตต์สเบิร์กรัฐเพนซิลเวเนียแจ็กสันเน้นย้ำถึงความสำคัญของการดูแลหลังผ่าตัด ซึ่งช่วยลดอัตราการเสียชีวิตลงอย่างมาก ภายในปี 1965 กายวิภาคศาสตร์ทางการผ่าตัดเป็นที่เข้าใจกันอย่างละเอียดและแพร่หลายยาปฏิชีวนะมีจำหน่ายอย่างแพร่หลายและมีประโยชน์ในการรักษาการติดเชื้อหลังผ่าตัด และภาวะแทรกซ้อนที่สำคัญอื่นๆ ก็สามารถจัดการได้ง่ายขึ้นเช่นกัน
สังคมและวัฒนธรรม
บุคคลที่มีชื่อเสียงที่ได้รับการผ่าตัดเจาะคอหรือเคยได้รับการผ่าตัดเจาะคอ ได้แก่Catherine Zeta-Jones , Mika Häkkinen , Stephen Hawking , Connie Culp , Christopher Reeve , [ 51 ] Roy Horn , William Rehnquist , Gabby Giffords , George Michael , Val Kilmer , [ 52 ]และอีกมากมาย[ 53 ]
ในภาพยนตร์และรายการโทรทัศน์หลายเรื่อง มีฉากที่ต้องทำการผ่าตัดฉุกเฉินที่คอเพื่อเปิดทางเดินหายใจใหม่ ตัวอย่างเช่น ในภาพยนตร์สยองขวัญเรื่องSaw V ปี 2008 ตัวละครที่กำลังจมน้ำถูกเจาะจากคอขึ้นไป ได้ทำการเจาะคอตัวเองด้วยปากกาเพื่อสร้างทางเดินหายใจให้หายใจได้ วิธีการที่พบได้บ่อยที่สุดคือ การเจาะ กระดูกอ่อนไทรอยด์ (cricothyrotomy หรือ crike) ซึ่งเป็นการกรีดผ่านผิวหนังและเยื่อหุ้มกระดูกอ่อนไทรอยด์ มักจะสับสนหรือเรียกผิดว่าเป็นการเจาะหลอดลม (tracheotomy หรือ trach) และในทางกลับกัน อย่างไรก็ตาม ทั้งสองวิธีแตกต่างกันอย่างมาก ขึ้นอยู่กับตำแหน่งของรูเปิดและระยะเวลาที่จำเป็นต้องใช้ทางเดินหายใจสำรอง
อีกตัวอย่างหนึ่งของการพยายามใช้ขั้นตอนดังกล่าวในกรณีฉุกเฉิน ปรากฏอยู่ในภาพยนตร์ตลกเรื่องThe Heat ปี 2013 โดย ตัวละครของ แซนดรา บุลล็อกในบทซาราห์ แอชเบิร์น พยายามทำการผ่าตัดช่วยคนสำลักแพนเค้กในร้านเดนนีส์แต่ไม่สำเร็จ จากนั้นตัวละครของ เมลิสซา แมคคาร์ธีในบทนักสืบมัลเลนส์ จึงกดลงบนหน้าอกของชายคนนั้นอย่างแรง ทำให้เศษอาหารหลุดออกจากปากของเขา
Further reading
- Plotnikow GA, Roux N, Feld V, Gogniat E, Villalba D, Ribero NV, Sartore M, Bosso M, Quiroga C, Leiva V, Scrigna M, Puchulu F, Distéfano E, Scapellato JL, Intile D, Planells F, Noval D, Buñirigo P, Jofré R, Nielsen ED (October 2013). "Evaluation of tracheal cuff pressure variation in spontaneously breathing patients". International Journal of Critical Illness and Injury Science. 3 (4): 262–8. doi:10.4103/2229-5151.124148. PMC 3891193. PMID 24459624.
External links
- Tracheotomy Info (A community for tracheotomy-wearers and the people who love them) at tracheotomy.info
- Tracheostomy Products and Support (Online resource for tracheostomy products, supplies and support) at trachs.com
- Aaron's tracheostomy page (Caring for a tracheostomy) at tracheostomy.com
- (Pictures with video clipping) at drtbalu.com
- Translaryngeal tracheostomyArchived 11 September 2017 at the Wayback Machine
- "Tracheotomy" at Dorland's Medical Dictionary
- Smiths Medical Tracheostomy Training Videos
- A Video of Rescue Breathing for Laryngectomees and Neck Breathers
- "Book of Simplification Concerning Therapeutics and Diet", is a manuscript from 1497 that discusses tracheotomies
- An all inclusive resource about tracheostomy including articles and courses for medical professionals, caregivers and patients
- Site and blog with information about tracheostomies
- Global Tracheostomy Collaborative. International collaborative with resources for hospitals, caregivers, and patients about tracheostomies, including international research
- Dilatational Tracheostomy On An Intensive Care Unit
สรุปเนื้อหา
ข้อมูลสำคัญจากบทความ
ข้อมูลสำคัญเกี่ยวกับ Tracheotomy
Tracheotomy (/ˌtreɪkiˈɒtəmi/, UK also/ˌtræki-/), or tracheostomy, is a surgical airway management procedure which consists of making an incision on the front of the neck to open a.
Etymology and terminology
The etymology of the word tracheotomy comes from two Greek words: the root tom- (from Greek τομή tomḗ ) meaning "to cut", and the word trachea (from Greek τραχεία tracheía ).
Indications
There are four main reasons why someone would receive a tracheotomy: [ 3 ]
Alternatives
Biphasic cuirass ventilation is a form of non-invasive mechanical ventilation that can — in a small subset of cases — allow people to avoid a tracheostomy. [ 6 ]