อ่าน 87 นาที
HIV/AIDS
The human immunodeficiency virus (HIV) is a retrovirus that attacks the immune system.
HIV/AIDS
| HIV/AIDS | |
|---|---|
| Other names | HIV disease, HIV infection[1][2] |
 | |
| The red ribbon is a symbol for solidarity with HIV-positive people and those living with AIDS.[3] | |
| Specialty | Infectious disease, immunology |
| Symptoms |
|
| Complications | Opportunistic infections, tumors[4] |
| Duration | Lifelong[4] |
| Causes | Human immunodeficiency virus (HIV)[4] |
| Risk factors | Unprotectedanal or vaginal sex, having another sexually transmitted infection, needle sharing, medical procedures involving unsterile cutting or piercing, and experiencing needlestick injury[4] |
| Diagnostic method | Blood tests[4] |
| Prevention | Safe sex, regular testing, voluntary male circumcision, needle and syringe programmes, pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP)[5] |
| Treatment | Antiretroviral drugs (ARVs)[4] |
| Prognosis | |
| Frequency | |
| Deaths | |
The human immunodeficiency virus (HIV)[8][9][10] is a retrovirus[11] that attacks the immune system. Without treatment, it can lead to a spectrum of conditions including acquired immunodeficiency syndrome (AIDS).[12] It is a preventable disease.[5] It can be managed with treatment and become a manageable chronic health condition.[5] While there is no cure or vaccine for HIV, antiretroviral treatment can slow the course of the disease, and, if used before significant disease progression, can extend the life expectancy of someone living with HIV to a nearly standard level.[5][13] An HIV-positive person on treatment can expect to live a normal life, and die with the virus, not of it.[12][13] Effective treatment for HIV-positive people (people living with HIV) involves a life-long regimen of medicine to suppress the virus, making the viral load undetectable. Early testing can show if treatment is needed to stop progression and to prevent infecting others.
Treatment is recommended as soon as the diagnosis is made.[14] An HIV-positive person who has an undetectable viral load as a result of long-term treatment has effectively no risk of transmitting HIV sexually.[15][16] Campaigns by UNAIDS and organizations around the world have communicated this as Undetectable = Untransmittable.[17]
Without treatment the infection can interfere with the immune system, and eventually progress to AIDS, sometimes taking many years. Following initial infection an individual may not notice any symptoms, or may experience a brief period of influenza-like illness.[4] During this period the person may not know that they are HIV-positive, yet they will be able to pass on the virus. Typically, this period is followed by a prolonged incubation period with no symptoms.[12] Eventually the HIV infection increases the risk of developing other infections such as tuberculosis, as well as other opportunistic infections, and tumors which are rare in people who have normal immune function.[4] The late stage is often also associated with unintended weight loss.[12] Without treatment, the life expectancy of an individual with HIV is around 11 years.[6]
HIV is spread primarily by unprotected sex (including anal, oral and vaginal sex), contaminated hypodermic needles or blood transfusions, and from mother to child during pregnancy, delivery, or breastfeeding.[18] Some bodily fluids, such as saliva, sweat, and tears, do not transmit the virus.[19]Oral sex has little risk of transmitting the virus.[20] Ways to avoid catching HIV and preventing the spread include safe sex, treatment to prevent infection ("PrEP"), treatment to stop infection in someone who has been recently exposed ("PEP"),[4]treating those who are infected, and needle exchange programs. Disease in a baby can often be prevented by giving both the mother and child antiretroviral medication.[4]
Recognized worldwide in the early 1980s,[21] HIV/AIDS has had a large impact on society, both as an illness and as a source of discrimination.[22] The disease also has large economic impacts.[22] There are many misconceptions about HIV/AIDS, such as the belief that it can be transmitted by casual non-sexual contact.[23] The disease has become subject to many controversies involving religion, including the Catholic Church's position not to support condom use as prevention.[24] It has attracted international medical and political attention as well as large-scale funding since it was identified in the 1980s.[25]
HIV made the jump from other primates to humans in west-central Africa in the early-to-mid-20th century.[26] AIDS was first recognized by the U.S. Centers for Disease Control and Prevention (CDC) in 1981 and its cause—HIV infection—was identified in the early part of the decade.[21] Between the first time AIDS was readily identified through 2024, the disease is estimated to have caused at least 42.3 million deaths worldwide.[5] In 2023, 630,000 people died from HIV-related causes, an estimated 1.3 million people acquired HIV and about 39.9 million people worldwide living with HIV, 65% of whom are in the World Health Organization (WHO) African Region.[5][7] HIV/AIDS is considered a pandemic—a disease outbreak which is present over a large area and is actively spreading.[27] The United States' National Institutes of Health (NIH) and the Gates Foundation have pledged $200 million focused on developing a global cure for AIDS.[28]
Signs and symptoms
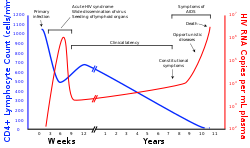
There are three main stages of HIV infection: acute infection, clinical latency, and AIDS.[1][29]
First main stage: acute infection

The initial period following infection with HIV is called acute HIV, primary HIV or acute retroviral syndrome.[29][30] Many individuals develop an influenza-like illness, mononucleosis or glandular fever 2–4 weeks after exposure while others have no significant symptoms.[31][32] Symptoms occur in 40–90% of cases and most commonly include fever, large tender lymph nodes, throat inflammation, a rash, headache, tiredness, and/or sores of the mouth and genitals.[30][32] The rash, which occurs in 20–50% of cases, presents itself on the trunk and is maculopapular, classically.[33] Some people also develop opportunistic infections at this stage.[30] Gastrointestinal symptoms, such as vomiting or diarrhea may occur.[32] Neurological symptoms of peripheral neuropathy or Guillain–Barré syndrome also occur.[32] The duration of the symptoms varies, but is usually one or two weeks.[32]
These symptoms are not often recognized as signs of HIV infection. Family doctors or hospitals can misdiagnose cases as one of the many common infectious diseases with similar symptoms. Someone with an unexplained fever who may have been recently exposed to HIV should consider testing to find out if they have been infected.[32]
Second main stage: clinical latency
The initial symptoms are followed by a stage called clinical latency, asymptomatic HIV, or chronic HIV.[1] Without treatment, this second stage of the natural history of HIV infection can last from about three years[34] to over 20 years[35] (on average, about eight years).[36] While typically there are few or no symptoms at first, near the end of this stage many people experience fever, weight loss, gastrointestinal problems and muscle pains.[1] Between 50% and 70% of people also develop persistent generalized lymphadenopathy, characterized by unexplained, non-painful enlargement of more than one group of lymph nodes (other than in the groin) for over three to six months.[29]
Although most HIV-1 infected individuals have a detectable viral load and in the absence of treatment will eventually progress to AIDS, a small proportion (about 5%) retain high levels of CD4+ T cells (T helper cells) without antiretroviral therapy for more than five years.[32][37] These individuals are classified as "HIV controllers" or long-term nonprogressors (LTNP).[37] Another group consists of those who maintain a low or undetectable viral load without anti-retroviral treatment, known as "elite controllers" or "elite suppressors". They represent approximately 1 in 300 infected persons.[38]
Third main stage: AIDS

Acquired immunodeficiency syndrome (AIDS) is defined as an HIV infection with either a CD4+ T cell count below 0.2 cells per mL or the occurrence of specific diseases associated with HIV infection.[32] In the absence of specific treatment, around half of people infected with HIV develop AIDS within ten years.[32] The most common initial conditions that alert to the presence of AIDS are pneumocystis pneumonia (40%), cachexia in the form of HIV wasting syndrome (20%), and esophageal candidiasis.[32] Other common signs include recurrent respiratory tract infections.[32]
Opportunistic infections may be caused by bacteria, viruses, fungi, and parasites that are normally controlled by the immune system.[39] Which infections occur depends partly on what organisms are common in the person's environment.[32] These infections may affect nearly every organ system.[40]
People with AIDS have an increased risk of developing various viral-induced cancers, including Kaposi's sarcoma, Burkitt's lymphoma, primary central nervous system lymphoma, and cervical cancer.[33] Kaposi's sarcoma is the most common cancer, occurring in 10% to 20% of people with HIV.[41] The second-most common cancer is lymphoma, which is the cause of death of nearly 16% of people with AIDS and is the initial sign of AIDS in 3% to 4%.[41] Both these cancers are associated with human herpesvirus 8 (HHV-8).[41] Cervical cancer occurs more frequently in those with AIDS because of its association with human papillomavirus (HPV).[41]Conjunctival cancer (of the layer that lines the inner part of eyelids and the white part of the eye) is also more common in those with HIV.[42]
Additionally, people with AIDS frequently have systemic symptoms such as prolonged fevers, sweats (particularly at night), swollen lymph nodes, chills, weakness, and unintended weight loss.[43] Diarrhea is another common symptom, present in about 90% of people with AIDS.[44] They can also be affected by diverse psychiatric and neurological symptoms independent of opportunistic infections and cancers.[45]
Transmission
| Exposure route | Chance of infection | |||
|---|---|---|---|---|
| Blood transfusion | 90%[46] | |||
| Childbirth (to child) | 25% without treatment;1–2% with antiretroviral treatment[47] | |||
| Needle-sharing injection drug use | 0.67%[48] | |||
| Percutaneous needle stick | 0.30%[49] | |||
| Receptive anal intercourse* | 0.04–3.0% [ 50 ] | |||
| การสอดใส่ทางทวารหนัก* | 0.03% [ 51 ] | |||
| การสอดใส่ทางช่องคลอดและอวัยวะเพศชาย* | 0.05–0.30% [ 50 ] [ 52 ] | |||
| การสอดใส่องคชาตเข้าสู่ช่องคลอด* | 0.01–0.38% [ 50 ] [ 52 ] | |||
| การมีเพศสัมพันธ์ทางปากแบบรับ*§ | 0–0.04% [ 50 ] | |||
| การสอดใส่ทางปาก*§ | 0–0.005% [ 53 ] | |||
| *สมมติว่าไม่ได้ใช้ถุงยางอนามัย §แหล่งที่มาหมายถึงการร่วมเพศทางปากที่กระทำกับผู้ชาย | ||||
เชื้อเอชไอวีแพร่กระจายได้ 3 ช่องทางหลัก ได้แก่การมีเพศสัมพันธ์การสัมผัสกับของเหลวหรือเนื้อเยื่อในร่างกายที่ติดเชื้อในปริมาณมาก และจากแม่สู่ลูกระหว่างตั้งครรภ์ คลอด หรือให้นมบุตร (เรียกว่าการถ่ายทอดทางแนวตั้ง ) [ 18 ]ไม่มีความเสี่ยงต่อการติดเชื้อเอชไอวีหากสัมผัสกับอุจจาระ น้ำมูกน้ำลายเสมหะเหงื่อ น้ำตา ปัสสาวะ หรืออาเจียน เว้นแต่ว่าสิ่งเหล่านี้จะปนเปื้อนเลือด[ 54 ]นอกจากนี้ยังสามารถติดเชื้อเอชไอวีมากกว่าหนึ่งสายพันธุ์พร้อมกันได้ ซึ่งเป็นภาวะที่เรียกว่าการติดเชื้อเอชไอวีซ้ำซ้อน[ 55 ]
เรื่องเพศ
วิธีการแพร่เชื้อ HIV ที่พบบ่อยที่สุดคือการมีเพศสัมพันธ์กับผู้ติดเชื้อ[ 18 ]อย่างไรก็ตาม ผู้ติดเชื้อ HIV ที่มีปริมาณไวรัสต่ำจนตรวจไม่พบอันเป็นผลมาจากการรักษาระยะยาว จะไม่มีความเสี่ยงในการแพร่เชื้อ HIV ทางเพศสัมพันธ์ ซึ่งเรียกว่าตรวจไม่พบ = แพร่เชื้อไม่ได้ [ 15 ] [ 16 ] การมีอยู่ของผู้ติดเชื้อ HIV ที่ไม่สามารถแพร่เชื้อได้เมื่อได้รับการรักษาด้วยยาต้านไวรัสได้รับการเผยแพร่อย่างเป็นที่ถกเถียงในแถลงการณ์ของสวิตเซอร์แลนด์ ปี 2008 และต่อมาได้รับการยอมรับว่าถูกต้องตามหลักการแพทย์[ 56 ]
ในระดับโลก รูปแบบการแพร่เชื้อเอชไอวีที่พบบ่อยที่สุดคือการมีเพศสัมพันธ์ระหว่างคนต่างเพศ [ 18 ] อย่างไรก็ตามรูปแบบการแพร่เชื้อจะแตกต่างกันไปในแต่ละประเทศ ณ ปี 2017 การแพร่เชื้อเอชไอวีส่วนใหญ่ในสหรัฐอเมริกาเกิดขึ้นในกลุ่มชายที่มีเพศสัมพันธ์กับชาย (ร้อยละ 82 ของการวินิจฉัยเอชไอวีรายใหม่ในกลุ่มชายอายุ 13 ปีขึ้นไป และร้อยละ 70 ของการวินิจฉัยรายใหม่ทั้งหมด) [ 57 ] [ 58 ]ในสหรัฐอเมริกา ชายรักร่วมเพศและชายรักสองเพศอายุ 13 ถึง 24 ปี คิดเป็นประมาณร้อยละ 92 ของการวินิจฉัยเอชไอวีรายใหม่ในกลุ่มชายทั้งหมดในกลุ่มอายุเดียวกัน และร้อยละ 27 ของการวินิจฉัยรายใหม่ในกลุ่มชายรักร่วมเพศและชายรักสองเพศทั้งหมด[ 59 ]
ในส่วนของ การมีเพศสัมพันธ์ต่างเพศ โดยไม่ป้องกันการประเมินความเสี่ยงของการแพร่เชื้อเอชไอวีต่อการมีเพศสัมพันธ์แต่ละครั้งดูเหมือนจะสูงกว่าในประเทศที่มีรายได้ต่ำถึงสี่ถึงสิบเท่าเมื่อเทียบกับประเทศที่มีรายได้สูง[ 60 ]ในประเทศที่มีรายได้ต่ำ ความเสี่ยงของการแพร่เชื้อจากหญิงสู่ชายอยู่ที่ประมาณ 0.38% ต่อการมีเพศสัมพันธ์หนึ่งครั้ง และการแพร่เชื้อจากชายสู่หญิงอยู่ที่ประมาณ 0.30% ต่อการมีเพศสัมพันธ์หนึ่งครั้ง ในขณะที่การประเมินที่เทียบเท่ากันสำหรับประเทศที่มีรายได้สูงอยู่ที่ 0.04% ต่อการมีเพศสัมพันธ์หนึ่งครั้งสำหรับการแพร่เชื้อจากหญิงสู่ชาย และ 0.08% ต่อการมีเพศสัมพันธ์หนึ่งครั้งสำหรับการแพร่เชื้อจากชายสู่หญิง[ 60 ]ความเสี่ยงของการแพร่เชื้อจากการมีเพศสัมพันธ์ทางทวารหนักนั้นสูงเป็นพิเศษ โดยประมาณอยู่ที่ 1.4–1.7% ต่อการมีเพศสัมพันธ์หนึ่งครั้งทั้งในเพศสัมพันธ์ต่างเพศและเพศสัมพันธ์ระหว่างเพศเดียวกัน[ 60 ] [ 61 ]ในขณะที่ความเสี่ยงของการแพร่เชื้อจากการมีเพศสัมพันธ์ทางปากนั้นค่อนข้างต่ำ แต่ก็ยังมีอยู่[ 62 ]ความเสี่ยงจากการรับการมีเพศสัมพันธ์ทางปากนั้นถูกอธิบายว่า "แทบไม่มีเลย" [ 63 ]อย่างไรก็ตาม มีรายงานเพียงไม่กี่กรณี[ 64 ]ความเสี่ยงต่อครั้งโดยประมาณอยู่ที่ 0–0.04% สำหรับการมีเพศสัมพันธ์ทางปากแบบรับ[ 65 ]ในสถานการณ์ที่เกี่ยวข้องกับการค้าประเวณีในประเทศที่มีรายได้ต่ำ ความเสี่ยงของการแพร่เชื้อจากหญิงสู่ชายโดยประมาณอยู่ที่ 2.4% ต่อครั้ง และการแพร่เชื้อจากชายสู่หญิงอยู่ที่ 0.05% ต่อครั้ง[ 60 ]
Risk of transmission increases in the presence of many sexually transmitted infections[66] and genital ulcers.[60] Genital ulcers increase the risk approximately fivefold.[60] Other sexually transmitted infections, such as gonorrhea, chlamydia, trichomoniasis, and bacterial vaginosis, are associated with somewhat smaller increases in risk of transmission.[65]
The viral load of an infected person is an important risk factor in both sexual and mother-to-child transmission.[67] During the first 2.5 months of an HIV infection, a person's infectiousness is twelve times higher due to the high viral load associated with acute HIV.[65] If the person is in the late stages of infection, rates of transmission are approximately eightfold greater.[60]
Commercial sex workers (including those in pornography) have an increased likelihood of contracting HIV.[68][69] Rough sex can be a factor associated with an increased risk of transmission.[70]Sexual assault is also believed to carry an increased risk of HIV transmission, as condoms are rarely worn, physical trauma to the vagina or rectum is likely, and there may be a greater risk of concurrent sexually transmitted infections.[71]
Body fluids

The second-most frequent mode of HIV transmission is via blood and blood products.[18] Blood-borne transmission can be through needle-sharing during intravenous drug use, needle-stick injury, transfusion of contaminated blood or blood product, or medical injections with unsterilized equipment. The risk from sharing a needle during drug injection is between 0.63% and 2.4% per act, with an average of 0.8%.[72] The risk of acquiring HIV from a needle stick from an HIV-infected person is estimated as 0.3% (about 1 in 333) per act and the risk following mucous membrane exposure to infected blood as 0.09% (about 1 in 1000) per act.[54] This risk may, however, be up to 5% if the introduced blood was from a person with a high viral load and the cut was deep.[73] In the United States, intravenous drug users made up 12% of all new cases of HIV in 2009,[74] and in some areas more than 80% of people who inject drugs are predicted to be HIV-positive.[18]
HIV is transmitted in about 90% of blood transfusions using infected blood.[46] In developed countries the risk of acquiring HIV from a blood transfusion is extremely low (less than one in half a million) where improved donor selection and HIV screening is performed;[18] for example, in the UK the risk was reported at one in five million in 2011[75] and in the United States it was one in 1.5 million in 2008.[76] In low-income countries, only half of transfusions may be appropriately screened (as of 2008),[77] and it is estimated that up to 15% of HIV infections in these areas come from transfusion of infected blood and blood products, representing between 5% and 10% of global infections.[18][78] It is possible to acquire HIV from organ and tissue transplantation, although this is rare because of screening.[79]
Unsafe medical injections play a role in HIV spread in sub-Saharan Africa. In 2007, between 12% and 17% of infections in this region were attributed to medical syringe use.[80] The World Health Organization estimates the risk of transmission as a result of a medical injection in Africa at 1.2%.[80] Risks are also associated with invasive procedures, assisted delivery, and dental care in this area of the world.[80]
People giving or receiving tattoos, piercings, and scarification are theoretically at risk of infection but no confirmed cases have been documented.[81] It is not possible for mosquitoes or other insects to transmit HIV.[82]
Mother-to-child
HIV can be transmitted from mother to child during pregnancy, during delivery, or through breast milk, resulting in the baby also contracting HIV.[18][83] As of 2008, vertical transmission accounted for about 90% of cases of HIV in children.[84] In the absence of treatment, the risk of transmission before or during birth is around 20%, and in those who also breastfeed 35%.[84] Treatment decreases this risk to less than 5%.[85]
Antiretrovirals when taken by either the mother or the baby decrease the risk of transmission in those who do breastfeed.[86] If blood contaminates food during pre-chewing it may pose a risk of transmission.[81] If a woman is untreated, two years of breastfeeding results in an HIV/AIDS risk in her baby of about 17%.[87] Due to the increased risk of death without breastfeeding in many areas in the developing world, the World Health Organization recommends either exclusive breastfeeding or the provision of safe formula.[87] All women known to be HIV-positive should be taking lifelong antiretroviral therapy.[87]
Virology
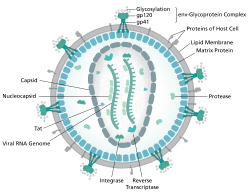

เชื้อ HIVเป็นสาเหตุของโรคที่เรียกว่า HIV/AIDS HIV เป็นเรโทรไวรัสที่ติดเชื้อส่วนประกอบของระบบภูมิคุ้มกัน ของมนุษย์เป็นหลัก เช่นเซลล์ CD4 + T, แมโครฟาจและเซลล์เดนดริติก มันทำลาย เซลล์ CD4 + T ทั้งทางตรงและทางอ้อม[ 88 ]
ไวรัส HIV เป็นสมาชิกของสกุลLentivirus [ 89 ] ซึ่งเป็นส่วนหนึ่งของวงศ์ Retroviridae [ 90 ] Lentivirus มีลักษณะทางสัณฐานวิทยาและชีววิทยา ร่วมกันหลายประการ สัตว์เลี้ยงลูกด้วยนมหลายชนิดติดเชื้อไวรัส Lentivirus ซึ่งโดยทั่วไปเป็นสาเหตุของโรคเรื้อรังที่มีระยะฟักตัวนาน[ 91 ] Lentivirus แพร่กระจายในรูปของ ไวรัส RNAสายเดี่ยวที่มีทิศทาง บวก และมีเปลือกหุ้มเมื่อเข้าสู่เซลล์เป้าหมายจีโนม RNA ของไวรัสจะถูกแปลง (ถอดรหัสย้อนกลับ) เป็น DNAสองสายโดยเอนไซม์reverse transcriptase ที่เข้ารหัสโดยไวรัส ซึ่งถูกขนส่งไปพร้อมกับจีโนมของไวรัสในอนุภาคไวรัส จากนั้น DNA ของไวรัสที่ได้จะถูกนำเข้าสู่นิวเคลียสของเซลล์และรวมเข้ากับ DNA ของเซลล์โดยเอนไซม์integrase ที่เข้ารหัสโดยไวรัส และปัจจัยร่วมของโฮสต์[ 92 ]เมื่อรวมเข้าด้วยกันแล้ว ไวรัสอาจอยู่ในสภาวะแฝงทำให้ไวรัสและเซลล์โฮสต์สามารถหลีกเลี่ยงการตรวจจับโดยระบบภูมิคุ้มกันได้[ 93 ]อีกทางเลือกหนึ่ง ไวรัสอาจถูกถอดรหัสทำให้เกิดจีโนม RNA ใหม่และโปรตีนไวรัสที่ถูกบรรจุและปล่อยออกจากเซลล์เป็นอนุภาคไวรัสใหม่ที่เริ่มต้นวงจรการจำลองแบบใหม่อีกครั้ง[ 94 ]
HIV is now known to spread between CD4+ T cells by two parallel routes: cell-free spread and cell-to-cell spread, i.e. it employs hybrid spreading mechanisms.[95] In the cell-free spread, virus particles bud from an infected T cell, enter the blood/extracellular fluid and then infect another T cell following a chance encounter.[95] HIV can also disseminate by direct transmission from one cell to another by a process of cell-to-cell spread.[96][97] The hybrid spreading mechanisms of HIV contribute to the virus' ongoing replication against antiretroviral therapies.[95][98]
Two types of HIV have been characterized: HIV-1 and HIV-2. HIV-1 is the virus that was originally discovered (and initially referred to also as LAV or HTLV-III). It is more virulent, more infective,[99] and is the cause of the majority of HIV infections globally. The lower infectivity of HIV-2 as compared with HIV-1 implies that fewer people exposed to HIV-2 will be infected per exposure. Because of its relatively poor capacity for transmission, HIV-2 is largely confined to West Africa.[100]
Pathophysiology

After the virus enters the body, there is a period of rapid viral replication, leading to an abundance of virus in the peripheral blood. During primary infection, the level of HIV may reach several million virus particles per milliliter of blood.[101] This response is accompanied by a marked drop in the number of circulating CD4+ T cells. The acute viremia is almost invariably associated with activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts recover. A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus.[102]
ในที่สุด เชื้อ HIV ก่อให้เกิดโรคเอดส์โดยการลดจำนวนเซลล์ CD4 + T ซึ่งทำให้ระบบภูมิคุ้มกันอ่อนแอลงและทำให้เกิดการติดเชื้อฉวยโอกาสได้เซลล์ T มีความสำคัญต่อการตอบสนองทางภูมิคุ้มกัน และหากไม่มีเซลล์ T ร่างกายจะไม่สามารถต่อสู้กับการติดเชื้อหรือฆ่าเซลล์มะเร็งได้ กลไกการลดจำนวนเซลล์ CD4 + T นั้นแตกต่างกันในระยะเฉียบพลันและระยะเรื้อรัง[ 103 ]ในระยะเฉียบพลัน การสลายตัวของเซลล์ที่เกิดจากเชื้อ HIV และการฆ่าเซลล์ที่ติดเชื้อโดยเซลล์ CD8 + T เป็นสาเหตุของการลดจำนวนเซลล์ CD4 + T แม้ว่าอะพอพโทซิสอาจเป็นปัจจัยหนึ่งด้วย ในระยะเรื้อรัง ผลที่ตามมาของการกระตุ้นภูมิคุ้มกันโดยทั่วไปควบคู่กับการสูญเสียความสามารถของระบบภูมิคุ้มกันในการสร้างเซลล์ T ใหม่ทีละน้อย ดูเหมือนจะเป็นสาเหตุของการลดลงอย่างช้าๆ ของจำนวนเซลล์ CD4 + T [ 104 ]
แม้ว่าอาการของภาวะภูมิคุ้มกันบกพร่องที่เป็นลักษณะเฉพาะของโรคเอดส์จะไม่ปรากฏให้เห็นเป็นเวลาหลายปีหลังจากที่บุคคลติดเชื้อ แต่การสูญเสียเซลล์ CD4 + T ส่วนใหญ่เกิดขึ้นในช่วงสัปดาห์แรกของการติดเชื้อ โดยเฉพาะอย่างยิ่งในเยื่อบุลำไส้ ซึ่งเป็นที่อยู่ของลิมโฟไซต์ส่วนใหญ่ที่พบในร่างกาย[ 105 ]เหตุผลของการสูญเสียเซลล์ CD4 + T ในเยื่อบุอย่างเป็นพิเศษก็คือ เซลล์ CD4 + T ในเยื่อบุส่วนใหญ่แสดง โปรตีน CCR5ซึ่งไวรัส HIV ใช้เป็นตัวรับร่วมเพื่อเข้าถึงเซลล์ ในขณะที่เซลล์ CD4 + T ในกระแสเลือดมีเพียงส่วนน้อยเท่านั้นที่ทำเช่นนั้น[ 106 ]การเปลี่ยนแปลงทางพันธุกรรมเฉพาะที่เปลี่ยนแปลงโปรตีน CCR5 เมื่อมีอยู่ในโครโมโซม ทั้งสอง จะป้องกันการติดเชื้อ HIV-1 ได้อย่างมีประสิทธิภาพมาก[ 107 ]
ในระหว่างการติดเชื้อเฉียบพลัน ไวรัสเอชไอวีจะค้นหาและทำลายเซลล์ CD4 + T ที่แสดงออก CCR5 [ 108 ]ในที่สุดการตอบสนองทางภูมิคุ้มกันที่รุนแรงจะควบคุมการติดเชื้อและเริ่มต้นระยะแฝงทางคลินิก เซลล์ CD4 + T ในเนื้อเยื่อเยื่อบุยังคงได้รับผลกระทบเป็นพิเศษ[ 108 ]การจำลองแบบของไวรัสเอชไอวีอย่างต่อเนื่องทำให้เกิดสภาวะการกระตุ้นภูมิคุ้มกันทั่วไปที่คงอยู่ตลอดระยะเรื้อรัง[ 109 ]การกระตุ้นภูมิคุ้มกัน ซึ่งสะท้อนให้เห็นจากการเพิ่มขึ้นของสถานะการกระตุ้นของเซลล์ภูมิคุ้มกันและการปล่อยไซโตไคน์ ที่ก่อให้เกิดการอักเสบ เป็นผลมาจากกิจกรรมของผลิตภัณฑ์ยีน เอชไอวีหลายชนิด และการตอบสนองทางภูมิคุ้มกันต่อการจำลองแบบของไวรัสเอชไอวีอย่างต่อเนื่อง นอกจากนี้ยังเชื่อมโยงกับการแตกสลายของระบบการเฝ้าระวังภูมิคุ้มกันของเยื่อบุทางเดินอาหารที่เกิดจากการลดลงของเซลล์ CD4 + T ในเยื่อบุในช่วงระยะเฉียบพลันของโรค[ 110 ]
โรคตาที่เกี่ยวข้องกับเอชไอวี/เอดส์พบได้บ่อยในผู้ที่ติดเชื้อโรคนี้ทั่วโลก ในบรรดาโรคเหล่านี้ โรคจอประสาทตาอักเสบจากเอชไอวีเป็นภาวะที่พบได้บ่อยที่สุด[ 111 ]ภาวะนี้พบได้ในผู้ป่วยที่ติดเชื้อเอชไอวีร้อยละ 40 ถึง 60 [ 112 ]และยังเป็นสาเหตุที่พบบ่อยที่สุดของการสูญเสียการมองเห็นในผู้ป่วยเหล่านี้อีกด้วย[ 112 ]
การวินิจฉัย
| การตรวจเลือด | วัน |
|---|---|
| การทดสอบแอนติบอดี(การทดสอบแบบรวดเร็ว, ELISAรุ่นที่ 3) | 23–90 |
| การทดสอบแอนติบอดีและแอนติเจน p24 (ELISA รุ่นที่ 4) | 18–45 |
| พีซีอาร์ | 10–33 |
HIV/AIDS is diagnosed via laboratory testing and then staged based on the presence of certain signs or symptoms.[30] HIV screening is recommended by the United States Preventive Services Task Force for all people 15 years to 65 years of age, including all pregnant women.[114] Additionally, testing is recommended for those at high risk, which includes anyone diagnosed with a sexually transmitted illness.[33][114] In many areas of the world, a third of HIV carriers only discover they are infected at an advanced stage of the disease when AIDS or severe immunodeficiency has become apparent.[33]
HIV testing


Most people infected with HIV develop seroconverted (antigen-specific) antibodies within three to twelve weeks after the initial infection.[32] Diagnosis of primary HIV before seroconversion is done by measuring HIV-RNA or p24 antigen.[32] Positive results obtained by antibody or PCR testing are confirmed either by a different antibody or by PCR.[30]
Antibody tests in children younger than 18 months are typically inaccurate, due to the continued presence of maternal antibodies.[115] Thus HIV infection can only be diagnosed by PCR testing for HIV RNA or DNA, or via testing for the p24 antigen.[30] Much of the world lacks access to reliable PCR testing, and people in many places simply wait until either symptoms develop or the child is old enough for accurate antibody testing.[115] In sub-Saharan Africa between 2007 and 2009, between 30% and 70% of the population were aware of their HIV status.[116] In 2009, between 3.6% and 42% of men and women in sub-Saharan countries were tested;[116] this represented a significant increase compared to previous years.[116]
Classifications
Two main clinical staging systems are used to classify HIV and HIV-related disease for surveillance purposes: the WHO disease staging system for HIV infection and disease,[30] and the CDC classification system for HIV infection.[117] The CDC's classification system is more frequently adopted in developed countries. Since the WHO's staging system does not require laboratory tests, it is suited to the resource-restricted conditions encountered in developing countries, where it can also be used to help guide clinical management. Despite their differences, the two systems allow a comparison for statistical purposes.[29][30][117]
The World Health Organization first proposed a definition for AIDS in 1986.[30] Since then, the WHO classification has been updated and expanded several times, with the most recent version being published in 2007.[30] The WHO system uses the following categories:
- Primary HIV infection: May be either asymptomatic or associated with acute retroviral syndrome[30]
- Stage I: HIV infection is asymptomatic with a CD4+ T cell count (also known as CD4 count) greater than 500 per microlitre (μL or cubic mm) of blood.[30] May include generalized lymph node enlargement.[30]
- Stage II: Mild symptoms, which may include minor mucocutaneous manifestations and recurrent upper respiratory tract infections. A CD4 count of less than 500/μL[30]
- Stage III: Advanced symptoms, which may include unexplained chronic diarrhea for longer than a month, severe bacterial infections including tuberculosis of the lung, and a CD4 count of less than 350/μL[30]
- Stage IV or AIDS: severe symptoms, which include toxoplasmosis of the brain, candidiasis of the esophagus, trachea, bronchi, or lungs, and Kaposi's sarcoma. A CD4 count of less than 200/μL[30]
The U.S. Centers for Disease Control and Prevention also created a classification system for HIV, and updated it in 2008 and 2014.[117][118] This system classifies HIV infections based on CD4 count and clinical symptoms, and describes the infection in five groups.[118] In those greater than six years of age it is:[118]
- Stage 0: the time between a negative or indeterminate HIV test followed less than 180 days by a positive test
- Stage 1: CD4 count ≥ 500 cells/μL and no AIDS-defining conditions
- Stage 2: CD4 count 200 to 500 cells/μL and no AIDS-defining conditions
- Stage 3: CD4 count ≤ 200 cells/μL or AIDS-defining conditions
- Unknown: if insufficient information is available to make any of the above classifications.
For surveillance purposes, the AIDS diagnosis still stands even if, after treatment, the CD4+ T cell count rises to above 200 per μL of blood or other AIDS-defining illnesses are cured.[29]
Prevention

Sexual contact

Consistent condom use reduces the risk of HIV transmission by approximately 80% over the long term.[119] When condoms are used consistently by a couple in which one person is infected, the rate of HIV infection is less than 1% per year.[120] There is some evidence to suggest that female condoms may provide an equivalent level of protection.[121] Application of a vaginal gel containing tenofovir (a reverse transcriptase inhibitor) immediately before sex seems to reduce infection rates by approximately 40% among African women.[122] By contrast, use of the spermicidenonoxynol-9 may increase the risk of transmission due to its tendency to cause vaginal and rectal irritation.[123]
Circumcision in sub-Saharan Africa "reduces the acquisition of HIV by heterosexual men by between 38% and 66% over 24 months".[124] Owing to these studies, both the World Health Organization and UNAIDS recommended male circumcision in 2007 as a method of preventing female-to-male HIV transmission in areas with high rates of HIV.[125] However, whether it protects against male-to-female transmission is disputed,[126][127] and whether it is of benefit in developed countries and among men who have sex with men is undetermined.[128][129][130]
Programs encouraging sexual abstinence do not appear to affect subsequent HIV risk.[131] Evidence of any benefit from peer education is equally poor.[132] Comprehensive sexual education provided at school may decrease high-risk behavior.[133][134] A substantial minority of young people continues to engage in high-risk practices despite knowing about HIV/AIDS, underestimating their own risk of becoming infected with HIV.[135] Voluntary counseling and testing people for HIV does not affect risky behavior in those who test negative but does increase condom use in those who test positive.[136] Enhanced family planning services appear to increase the likelihood of women with HIV using contraception, compared to basic services.[137] It is not known whether treating other sexually transmitted infections is effective in preventing HIV.[66]
Pre-exposure
Antiretroviral treatment among people with HIV whose CD4 count ≤ 550 cells/μL is a very effective way to prevent HIV infection of their partner (a strategy known as treatment as prevention, or TASP).[138] TASP is associated with a 10- to 20-fold reduction in transmission risk.[138][139]Pre-exposure prophylaxis for HIV ("PrEP") with a daily dose of the medications tenofovir, with or without emtricitabine, is effective in people at high risk including men who have sex with men, couples where one is HIV-positive, and young heterosexuals in Africa.[122][140] It may also be effective in intravenous drug users, with a study finding a decrease in risk of 0.7 to 0.4 per 100 person years.[141] The USPSTF, in 2019, recommended PrEP in those who are at high risk.[142]
Universal precautions within the health care environment are believed to be effective in decreasing the risk of HIV.[143]Intravenous drug use is an important risk factor, and harm reduction strategies such as needle-exchange programs and opioid substitution therapy appear effective in decreasing this risk.[144][145]
Post-exposure
A course of antiretrovirals administered within 48 to 72 hours after exposure to HIV-positive blood or genital secretions is referred to as post-exposure prophylaxis (PEP).[146] The use of the single agent zidovudine reduces the risk of an HIV infection five-fold following a needle-stick injury.[146] As of 2013, the prevention regimen recommended in the United States consists of three medications—tenofovir, emtricitabine and raltegravir—as this may reduce the risk further.[147]
PEP treatment is recommended after a sexual assault when the perpetrator is known to be HIV-positive, but is controversial when their HIV status is unknown.[148] The duration of treatment is usually four weeks[149] and is frequently associated with adverse effects—where zidovudine is used, about 70% of cases result in adverse effects such as nausea (24%), fatigue (22%), emotional distress (13%) and headaches (9%).[54]
Mother-to-child
Programs to prevent the vertical transmission of HIV (from mothers to children) can reduce rates of transmission by 92–99%.[84][144] This primarily involves the use of a combination of antiviral medications during pregnancy and after birth in the infant, and potentially includes bottle feeding rather than breastfeeding.[84][150] If replacement feeding is acceptable, feasible, affordable, sustainable and safe, mothers should avoid breastfeeding their infants; however, exclusive breastfeeding is recommended during the first months of life if this is not the case.[151] If exclusive breastfeeding is carried out, the provision of extended antiretroviral prophylaxis to the infant decreases the risk of transmission.[152] In 2015, Cuba became the first country in the world to eradicate mother-to-child transmission of HIV.[153]
Vaccination
Currently there is no licensed vaccine for HIV or AIDS.[13] The most effective vaccine trial to date, RV 144, was published in 2009; it found a partial reduction in the risk of transmission of roughly 30%, stimulating some hope in the research community of developing a truly effective vaccine.[154]
Treatment
HIV/AIDS is a chronic condition, as there is currently no cure. Treatment consists of highly active antiretroviral therapy (ART), which slows progression of the disease.[155] As of 2022, 39 million people globally were living with HIV, and 29.8 million people were accessing ART.[156] Treatment also includes preventive and active treatment of opportunistic infections. As of July 2022, four people have been successfully cleared of HIV.[157][158][159] Rapid initiation of antiretroviral therapy within one week of diagnosis appear to improve treatment outcomes in low and medium-income settings and is recommend for newly diagnosed HIV patients.[160][161]
HIV retinopathy was a very common cause of blindness in people with AIDS before the introduction of highly active antiretroviral therapy, but its incidence is declining due to proper and timely management of AIDS.[112] Even if there are signs of retinopathy, it may reverse as CD4+ T cell counts increase. Reversal of HIV retinopathy is a helpful sign of positive response to antiretroviral therapy in AIDS patients.[111] But if HIV treatment is delayed it may lead to permanent visual loss.[112]
Occurrence of HIV retinopathy may also be an indicator of therapeutic failure in AIDS patients undergoing treatment.[162]
Antiviral therapy

Current ART options are combinations (or "cocktails") consisting of at least three medications belonging to at least two types, or "classes", of antiretroviral agents.[163] There are eight classes of antiretroviral agents (ARVs), and over 30 individual drugs: nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase, inhibitors (NNRTIs), protease inhibitors (PIs), integrase strand transfer inhibitors (INSTIs), a fusion inhibitor, a CCR5 antagonist, a CD4 T lymphocyte (CD4) post-attachment inhibitor, and a gp120 attachment inhibitor. There are also two drugs, ritonavir (RTV) and cobicistat (COBI) which can be used as pharmacokinetic (PK) enhancers (or boosters) to improve the PK profiles of PIs and the INSTI elvitegravir (EVG).[164] Depending on the guidelines being followed, initial treatment generally consists of two nucleoside reverse transcriptase inhibitors along with a third ARV, either an integrase strand transfer inhibitor (INSTI), a non-nucleoside reverse transcriptase inhibitor (NNRTI), or a protease inhibitor with a pharmacokinetic enhancer (also known as a booster).[164]
The World Health Organization and the United States recommend antiretrovirals in people of all ages (including pregnant women) as soon as the diagnosis is made, regardless of CD4 count.[14][165][166] Once treatment is begun, it is recommended that it is continued without breaks or "holidays".[33] Many people are diagnosed only after treatment ideally should have begun.[33] The desired outcome of treatment is a long-term plasma HIV-RNA count below 50 copies/mL.[33] Levels to determine if treatment is effective are initially recommended after four weeks and once levels fall below 50 copies/mL checks every three to six months are typically adequate.[33] Inadequate control is deemed to be greater than 400 copies/mL.[33] Based on these criteria treatment is effective in more than 95% of people during the first year.[33]
Benefits of treatment include a decreased risk of progression to AIDS and a decreased risk of death.[167] In the developing world, treatment also improves physical and mental health.[168] With treatment, there is a 70% reduced risk of acquiring tuberculosis.[163] Additional benefits include a decreased risk of transmission of the disease to sexual partners and a decrease in mother-to-child transmission.[163][169] The effectiveness of treatment depends to a large part on compliance.[33] Reasons for non-adherence to treatment include poor access to medical care,[170] inadequate social supports, mental illness and drug abuse.[171] The complexity of treatment regimens (due to pill numbers and dosing frequency) and adverse effects may reduce adherence.[172] Even though cost is an important issue with some medications,[173] 47% of those who needed them were taking them in low- and middle-income countries as of 2010,[174] and the rate of adherence is similar in low-income and high-income countries.[175]
Specific adverse events are related to the antiretroviral agent taken.[176] Some relatively common adverse events include: lipodystrophy syndrome, dyslipidemia, and diabetes mellitus, especially with protease inhibitors.[29] Other common symptoms include diarrhea,[176][177] and an increased risk of cardiovascular disease.[178] Newer recommended treatments are associated with fewer adverse effects.[33] Certain medications may be associated with birth defects and therefore may be unsuitable for women hoping to have children.[33]
Treatment recommendations for children are somewhat different from those for adults. The World Health Organization recommends treating all children less than five years of age; children above five are treated like adults.[179] The United States guidelines recommend treating all children less than 12 months of age and all those with HIV RNA counts greater than 100,000 copies/mL between one year and five years of age.[180]
The European Medicines Agency (EMA) has recommended the granting of marketing authorizations for two new antiretroviral (ARV) medicines, rilpivirine (Rekambys) and cabotegravir (Vocabria), to be used together for the treatment of people with human immunodeficiency virus type 1 (HIV-1) infection.[181] The two medicines are the first ARVs that come in a long-acting injectable formulation.[181] This means that instead of daily pills, people receive intramuscular injections monthly or every two months.[181]
The combination of Rekambys and Vocabria injection is intended for maintenance treatment of adults who have undetectable HIV levels in the blood (viral load less than 50 copies/mL) with their current ARV treatment, and when the virus has not developed resistance to a certain class of anti-HIV medicines called non-nucleoside reverse transcriptase inhibitors (NNRTIs) and integrase strand transfer inhibitors (INIs).[181]
Cabotegravir combined with rilpivirine (Cabenuva) is a complete regimen for the treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults to replace a current antiretroviral regimen in those who are virologically suppressed on a stable antiretroviral regimen with no history of treatment failure and with no known or suspected resistance to either cabotegravir or rilpivirine.[182][183]
Opportunistic infections
Measures to prevent opportunistic infections are effective in many people with HIV/AIDS. In addition to improving current disease, treatment with antiretrovirals reduces the risk of developing additional opportunistic infections.[176]
Adults and adolescents who are living with HIV (even on anti-retroviral therapy) with no evidence of active tuberculosis in settings with high tuberculosis burden should receive isoniazid preventive therapy (IPT); the tuberculin skin test can be used to help decide if IPT is needed.[184] Children with HIV may benefit from screening for tuberculosis.[185]Vaccination against hepatitis A and B is advised for all people at risk of HIV before they become infected; however, it may also be given after infection.[186]
Trimethoprim/sulfamethoxazole prophylaxis between four and six weeks of age, and ceasing breastfeeding of infants born to HIV-positive mothers, is recommended in resource-limited settings.[187] It is also recommended to prevent PCP when a person's CD4 count is below 200 cells/uL and in those who have or have previously had PCP.[188] People with substantial immunosuppression are also advised to receive prophylactic therapy for toxoplasmosis and MAC.[189] Appropriate preventive measures reduced the rate of these infections by 50% between 1992 and 1997.[190]Influenza vaccination and pneumococcal polysaccharide vaccine are often recommended in people with HIV/AIDS with some evidence of benefit.[191][192]
Diet
The World Health Organization (WHO) has issued recommendations regarding nutrient requirements in HIV/AIDS.[193] A generally healthy diet is promoted. Dietary intake of micronutrients at RDA levels by HIV-infected adults is recommended by the WHO; higher intake of vitamin A, zinc, and iron can produce adverse effects in HIV-positive adults, and is not recommended unless there is documented deficiency.[193][194][195][196] Dietary supplementation for people who are infected with HIV and who have inadequate nutrition or dietary deficiencies may strengthen their immune systems or help them recover from infections; however, evidence indicating an overall benefit in morbidity or reduction in mortality is not consistent.[197]
People with HIV/AIDS are up to four times more likely to develop type 2 diabetes than those who are not tested positive with the virus.[198]
Evidence for supplementation with selenium is mixed with some tentative evidence of benefit.[199] For pregnant and lactating women with HIV, multivitamin supplement improves outcomes for both mothers and children.[200] If the pregnant or lactating mother has been advised to take anti-retroviral medication to prevent mother-to-child HIV transmission, multivitamin supplements should not replace these treatments.[200] There is some evidence that vitamin A supplementation in children with an HIV infection reduces mortality and improves growth.[201]
Alternative medicine
In the US, approximately 60% of people with HIV use various forms of complementary or alternative medicine,[202] whose effectiveness has not been established.[203] There is not enough evidence to support the use of herbal medicines.[204] There is insufficient evidence to recommend or support the use of medical cannabis to try to increase appetite or weight gain.[205]
Prognosis

HIV/AIDS has become a chronic rather than an acutely fatal disease in many areas of the world.[206] Prognosis varies between people, and both the CD4 count and viral load are useful for predicted outcomes.[32] Without treatment, average survival time after infection with HIV is estimated to be 9 to 11 years, depending on the HIV subtype.[6] After the diagnosis of AIDS, if treatment is not available, survival ranges between 6 and 19 months.[207][208]ART and appropriate prevention of opportunistic infections reduces the death rate by 80%, and raises the life expectancy for a newly diagnosed young adult to 20–50 years.[206][209][210] This is between two thirds[209] and nearly that of the general population.[33][211] If treatment is started late in the infection, prognosis is not as good:[33] for example, if treatment is begun following the diagnosis of AIDS, life expectancy is ~10–40 years.[33][206] Half of infants born with HIV die before two years of age without treatment.[187][212]

no data ≤ 10 10–25 25–50 50–100 | 100–500 500–1000 1,000–2,500 2,500–5,000 5,000–7500 | 7,500–10,000 10,000–50,000 ≥ 50,000 |
The primary causes of death from HIV/AIDS are opportunistic infections and cancer, both of which are frequently the result of the progressive failure of the immune system.[190][213] Risk of cancer appears to increase once the CD4 count is below 500/μL.[33] The rate of clinical disease progression varies widely between individuals and has been shown to be affected by a number of factors such as a person's susceptibility and immune function;[214] their access to health care, the presence of co-infections;[207][215] and the particular strain (or strains) of the virus involved.[216][217]
การติดเชื้อ วัณโรคร่วมด้วยเป็นหนึ่งในสาเหตุหลักของการเจ็บป่วยและเสียชีวิตในผู้ติดเชื้อเอชไอวี/เอดส์ โดยพบในผู้ติดเชื้อเอชไอวีหนึ่งในสาม และเป็นสาเหตุของการเสียชีวิตที่เกี่ยวข้องกับเอชไอวีถึง 25% [ 218 ]เอชไอวียังเป็นปัจจัยเสี่ยงที่สำคัญที่สุดอย่างหนึ่งของวัณโรค[ 219 ]ไวรัสตับอักเสบซีเป็นการติดเชื้อร่วมที่พบได้บ่อยมากอีกโรคหนึ่ง โดยแต่ละโรคจะเพิ่มความรุนแรงของอีกโรคหนึ่ง[ 220 ]มะเร็งที่พบได้บ่อยที่สุดสองชนิดที่เกี่ยวข้องกับเอชไอวี/เอดส์ ได้แก่มะเร็งคาโปซีซาร์โคมาและมะเร็งต่อมน้ำเหลืองชนิดนอนฮอดจ์กินที่เกี่ยวข้องกับเอดส์[ 213 ]มะเร็งชนิดอื่นๆ ที่พบได้บ่อยกว่า ได้แก่มะเร็งทวารหนักมะเร็งต่อมน้ำเหลืองเบอร์กิตมะเร็งต่อมน้ำ เหลือง ในระบบประสาทส่วนกลางและมะเร็งปากมดลูก[ 33 ] [ 221 ]
แม้จะ ได้ รับการรักษาด้วยยาต้านไวรัส แล้วในระยะยาวผู้ติดเชื้อเอชไอวีอาจประสบกับความผิดปกติทางระบบประสาทและสมอง[ 222 ] โรคกระดูกพรุน[ 223 ]โรคเส้นประสาท[ 224 ] โรคมะเร็ง [ 225 ] [ 226 ]โรคไต [ 227 ]และโรคหัวใจและหลอดเลือด [ 177 ] บางภาวะ เช่นโรคไขมันใต้ผิวหนังผิดปกติอาจเกิดจากทั้งเชื้อเอชไอวีและการรักษา[ 177 ]
ระบาดวิทยา


เอชไอวี/เอดส์ถือเป็นโรคระบาดระดับโลก[ 229 ]ณปี 2022 มีผู้ติดเชื้อเอชไอวีทั่วโลกประมาณ 39 ล้านคน โดยมีผู้ติดเชื้อรายใหม่ประมาณ 1.3 ล้านคนในปีนั้น[ 156 ]ซึ่งลดลงจาก 2.1 ล้านคนในปี 2010 [ 156 ]ในบรรดาผู้ติดเชื้อรายใหม่ 44% เป็นผู้หญิงและเด็กหญิงทั่วโลก[ 156 ]มีผู้เสียชีวิตจากโรคเอดส์ 630,000 รายในปี 2022 ลดลงจากจุดสูงสุดที่ 2 ล้านรายในปี 2005 [ 156 ]องค์การอนามัยโลกรายงานว่าการเสียชีวิตจากเอชไอวีและเอดส์ "ลดลง 61% จากสาเหตุการเสียชีวิตอันดับ 7 ของโลกในปี 2000 มาเป็นอันดับ 21 ในปี 2021" [ 230 ]
Among persons living with HIV (PLWH), the largest proportion reside in eastern and southern Africa (20.6 million, 54.6%). This region also had the highest rate of adult and child deaths due to AIDS in 2020 (310,000, 46.6%). Sub-Saharan African adolescent girls and young women (aged 15–24 years) account for 77% of new infections among this age-range globally.[156] Here, in contrast to other regions, adolescent girls and young women are three times more likely to acquire HIV than age-matched males.[156] Despite these statistics, overall, new HIV infections and AIDS-related deaths have substantially decreased in this region since 2010.[231]
Eastern Europe and central Asia has observed a 43% increase in new HIV infections and 32% increase in AIDS-related deaths since 2010, the highest of all global regions.[231] These infections are predominantly distributed in persons who inject drugs, with gay men and other men who have sex with men or persons who engage in transaction sex the second and third populations most impacted in this region.[231]
At the end of 2019, United States indicated that approximately 1.2 million people aged ≥13 years were living with HIV, resulting in about 18,500 deaths in 2020.[232] There were 34,800 estimated new infections in the US in 2019, 53% of which were in the southern region of the country.[232] In addition to geographic location, significant disparities in HIV incidence exist among men, Black or Hispanic populations, and men who reported male-to-male sexual contact. The US Centers for Disease Control and Prevention estimated that in that year, 158,500 people or 13% of infected Americans were unaware of their infection.[232]
ในสหราชอาณาจักรณ ปี 2015 มีผู้ป่วยประมาณ 101,200 ราย และเสียชีวิต 594 ราย[ 233 ]ในแคนาดา ณ ปี 2008 มีผู้ป่วยประมาณ 65,000 ราย และเสียชีวิต 53 ราย[ 234 ]ระหว่างการค้นพบโรคเอดส์ครั้งแรก (ในปี 1981) จนถึงปี 2009 มีผู้เสียชีวิตจากโรคนี้เกือบ 30 ล้านราย[ 235 ]อัตราการติดเชื้อ HIV ต่ำที่สุดในแอฟริกาเหนือและตะวันออกกลาง (0.1% หรือน้อยกว่า) เอเชียตะวันออก (0.1%) และยุโรปตะวันตกและกลาง (0.2%) [ 236 ]ประเทศในยุโรปที่ได้รับผลกระทบมากที่สุด ตามการประมาณการในปี 2009 และ 2012 ได้แก่รัสเซียยูเครนลัตเวีย มอลโดวาโปรตุเกสและเบลารุสตามลำดับความชุกที่ลดลง[ 237 ]
กลุ่มที่มีความเสี่ยงสูงต่อการติดเชื้อเอชไอวี ได้แก่ ผู้ที่มีส่วนร่วมในการค้าประเวณีเกย์และ ชาย อื่น ๆที่มีเพศสัมพันธ์กับชายผู้ที่ฉีดสารเสพติดบุคคลข้ามเพศและผู้ที่ถูกจำคุกหรือถูกควบคุมตัว[ 156 ]
การเปลี่ยนแปลงสภาพภูมิอากาศส่งผลกระทบต่อความเสี่ยงต่อการติดเชื้อเอชไอวีและความพร้อมใช้งานและการเข้าถึงบริการป้องกันและรักษาเอชไอวี และอาจส่งผลให้เกิดภาวะโภชนาการไม่ดี ภูมิคุ้มกันบกพร่อง และการไม่ปฏิบัติตามการรักษาอย่างเคร่งครัด[ 238 ] [ 239 ]
ประวัติศาสตร์
การค้นพบ

ข่าวเรื่องแรกเกี่ยวกับโรคนี้ปรากฏในหนังสือพิมพ์เกย์New York Nativeเมื่อ วันที่ 18 พฤษภาคม 1981 [ 240 ] [ 241 ]โรคเอดส์ได้รับการรายงานทางคลินิกครั้งแรกเมื่อวันที่ 5 มิถุนายน 1981 โดยมีผู้ป่วย 5 รายในสหรัฐอเมริกา[ 41 ] [ 242 ]ผู้ป่วยกลุ่มแรกเป็นกลุ่มผู้ใช้ยาเสพติดแบบฉีดและชายรักร่วมเพศที่ไม่มีสาเหตุของภูมิคุ้มกันบกพร่องที่ทราบแน่ชัด ซึ่งแสดงอาการของโรคปอดบวมจาก เชื้อ Pneumocystis carinii (PCP) ซึ่งเป็นการติดเชื้อฉวยโอกาสที่หายากและเป็นที่ทราบกันดีว่าเกิดขึ้นในผู้ที่มีระบบภูมิคุ้มกันบกพร่องอย่างมาก[ 243 ]หลังจากนั้นไม่นาน ชายรักร่วมเพศจำนวนมากก็เป็นมะเร็งผิวหนังที่หายากชนิดหนึ่งที่เรียกว่าKaposi's sarcoma (KS) [ 244 ] [ 245 ]มีผู้ป่วย PCP และ KS เพิ่มขึ้นอีกมากมาย ทำให้ศูนย์ควบคุมและป้องกันโรคแห่งสหรัฐอเมริกา (CDC) ตื่นตัว และมีการจัดตั้งคณะทำงานของ CDC เพื่อติดตามการระบาด[ 246 ]
ในช่วงแรก CDC ยังไม่มีชื่ออย่างเป็นทางการสำหรับโรคนี้ มักจะอ้างถึงโรคนี้โดยใช้ชื่อโรคที่เกี่ยวข้อง เช่น โรค ต่อมน้ำเหลืองโตซึ่งเป็นชื่อที่ผู้ค้นพบเชื้อ HIV ตั้งชื่อไวรัสในตอนแรก[ 247 ] [ 248 ]พวกเขายังใช้ชื่อKaposi's sarcoma และการติดเชื้อฉวยโอกาสซึ่งเป็นชื่อที่คณะทำงานถูกตั้งขึ้นในปี 1981 [ 249 ]ในช่วงหนึ่ง CDC เรียกโรคนี้ว่า "โรค 4H" เนื่องจากกลุ่มอาการนี้ดูเหมือนจะส่งผลกระทบต่อผู้ใช้เฮโรอีน กลุ่มรักร่วมเพศ ผู้ป่วยโรคฮีโมฟีเลียและชาวเฮติ [ 250 ] [ 251 ] นอกจากนี้ยังมีการบัญญัติคำว่าGRIDซึ่งย่อมาจากgay-related immune deficiency (ภาวะภูมิคุ้มกันบกพร่องที่เกี่ยวข้องกับเกย์) อีกด้วย [ 252 ]อย่างไรก็ตาม หลังจากที่พบว่าโรคเอดส์ไม่ได้จำกัดอยู่เฉพาะในกลุ่มคนรักร่วมเพศ [ 249 ]จึงตระหนักว่าคำว่าGRID นั้นทำให้เข้าใจผิด และได้มีการนำคำว่าAIDSมาใช้ในการประชุมเมื่อเดือนกรกฎาคม พ.ศ. 2525 [ 253 ]ภายในเดือนกันยายน พ.ศ. 2525 CDC จึงเริ่มเรียกโรคนี้ว่า AIDS [ 254 ]
การทบทวนประวัติศาสตร์ของการระบาดของโรคเอดส์เน้นย้ำว่าผู้ป่วยกลุ่มแรกมักมีผื่นขึ้นตามผิวหนังผิดปกติ ต่อมน้ำเหลืองโต และน้ำหนักลด ซึ่งเป็นสัญญาณที่ทำให้แพทย์สงสัยว่าเป็นโรคติดเชื้อชนิดใหม่ก่อนที่จะมีการระบุเชื้อเอชไอวี[ 255 ]การศึกษาทางคลินิกในช่วงแรกได้บันทึกอาการทางผิวหนังที่เป็นลักษณะเฉพาะของโรค ในปี 1985 แพทย์ผิวหนังชาวอังกฤษ Charles Farthing, Richard Staughton และChristopher Rowland Payneได้ตีพิมพ์คำอธิบายโดยละเอียดครั้งแรกเกี่ยวกับอาการทางผิวหนังในผู้ป่วยโรคเอดส์และการติดเชื้อ HTLV-III ซึ่งรวมถึงโรคผิวหนังอักเสบจากต่อมไขมัน โรครูขุมขนอักเสบ และรอยโรคหลอดเลือดอักเสบ[ 256 ]
ในปี พ.ศ. 2526 กลุ่มวิจัยสองกลุ่มที่แยกจากกัน นำโดยRobert GalloและLuc Montagnierประกาศว่าไวรัสเรโทรชนิดใหม่อาจติดเชื้อในผู้ป่วยเอดส์ และตีพิมพ์ผลการค้นพบของพวกเขาในวารสาร Science ฉบับเดียวกัน[ 257 ] [ 248 ] Gallo อ้างว่าไวรัสที่กลุ่มของเขาแยกได้จากผู้ป่วยเอดส์มีรูปร่าง คล้ายกับ ไวรัส T-lymphotropic ของมนุษย์ (HTLV) อื่นๆที่กลุ่มของเขาเป็นกลุ่มแรกที่แยกได้ กลุ่มของ Gallo เรียกไวรัสที่แยกได้ใหม่นี้ว่า HTLV-III ในเวลาเดียวกัน กลุ่มของ Montagnier ได้แยกไวรัสจากผู้ป่วยที่มีอาการบวมของต่อมน้ำเหลืองที่คอและอ่อนเพลียซึ่งเป็นอาการลักษณะเฉพาะสองอย่างของเอดส์ ซึ่งขัดแย้งกับรายงานจากกลุ่มของ Gallo Montagnier และเพื่อนร่วมงานของเขาแสดงให้เห็นว่าโปรตีนหลักของไวรัสนี้มีความแตกต่างทางภูมิคุ้มกันจาก HTLV-I กลุ่มของ Montagnier ตั้งชื่อไวรัสที่แยกได้ว่าไวรัสที่เกี่ยวข้องกับต่อมน้ำเหลืองโต (LAV) [ 246 ]เนื่องจากไวรัสทั้งสองชนิดนี้เป็นชนิดเดียวกัน ในปี พ.ศ. 2529 LAV และ HTLV-III จึงถูกเปลี่ยนชื่อเป็น HIV [ 258 ]
ต้นกำเนิด

ที่มาของเชื้อ HIV/AIDS และสถานการณ์ที่นำไปสู่การเกิดขึ้นของโรคนี้ยังคงไม่สามารถไขปริศนาได้[ 259 ]
เชื่อกันว่าทั้ง HIV-1 และ HIV-2 มีต้นกำเนิดมาจากไพรเมต ที่ไม่ใช่มนุษย์ ในแอฟริกาตะวันตกตอนกลาง และถูกถ่ายทอดมาสู่มนุษย์ในช่วงต้นศตวรรษที่ 20 [ 26 ]ดูเหมือนว่า HIV-1 จะมีต้นกำเนิดในแคเมรูน ตอนใต้ ผ่านวิวัฒนาการของ SIV(cpz) ซึ่งเป็น ไวรัสภูมิคุ้มกันบกพร่องในลิง (SIV) ที่ติดเชื้อในลิงชิมแปนซี ป่า (HIV-1 สืบเชื้อสายมาจาก SIVcpz ที่ระบาดในลิงชิมแปนซีสายพันธุ์ย่อย Pan troglodytes troglodytes ) [ 260 ] [ 261 ]ญาติที่ใกล้เคียงที่สุดของ HIV-2 คือ SIV (smm) ซึ่งเป็นไวรัสของลิงโซตี้แมงกาเบย์ ( Cercocebus atys atys ) ซึ่งเป็นลิงโลกเก่าที่อาศัยอยู่ในชายฝั่งแอฟริกาตะวันตก (จากเซเนกัล ตอนใต้ ถึงไอวอรี่โคสต์ ตะวันตก ) [ 100 ]ลิงโลกใหม่เช่นลิงนกฮูกมีความต้านทานต่อ การติดเชื้อ HIV-1อาจเป็นเพราะการหลอมรวม ทางพันธุกรรม ของยีนต้านทานไวรัสสองยีน[ 262 ]เชื่อกันว่า HIV-1 ได้ข้ามกำแพงสายพันธุ์อย่างน้อยสามครั้ง ทำให้เกิดไวรัสสามกลุ่ม ได้แก่ M, N และ O [ 263 ]
มีหลักฐานว่ามนุษย์ที่มีส่วนร่วมใน กิจกรรม เกี่ยวกับเนื้อสัตว์ป่าไม่ว่าจะเป็นนักล่าหรือผู้ขายเนื้อสัตว์ป่า มักจะติดเชื้อ SIV [ 264 ]อย่างไรก็ตาม SIV เป็นไวรัสที่อ่อนแอ ซึ่งโดยทั่วไปแล้วระบบภูมิคุ้มกันของมนุษย์จะยับยั้งได้ภายในไม่กี่สัปดาห์หลังการติดเชื้อ เชื่อกันว่าจำเป็นต้องมีการแพร่เชื้อไวรัสจากบุคคลหนึ่งไปยังอีกบุคคลหนึ่งหลายครั้งติดต่อกันอย่างรวดเร็ว เพื่อให้ไวรัสมีเวลาเพียงพอที่จะกลายพันธุ์เป็น HIV [ 265 ]นอกจากนี้ เนื่องจากอัตราการแพร่เชื้อจากคนสู่คนค่อนข้างต่ำ SIV จึงสามารถแพร่กระจายไปทั่วประชากรได้ก็ต่อเมื่อมีช่องทางการแพร่เชื้อที่มีความเสี่ยงสูงอย่างน้อยหนึ่งช่องทาง ซึ่งเชื่อกันว่าไม่มีอยู่ในแอฟริกาก่อนศตวรรษที่ 20 [ 266 ]
ช่องทางการแพร่เชื้อที่มีความเสี่ยงสูงที่เสนอไว้โดยเฉพาะ ซึ่งทำให้ไวรัสสามารถปรับตัวเข้ากับมนุษย์และแพร่กระจายไปทั่วสังคมนั้น ขึ้นอยู่กับช่วงเวลาที่เสนอของการแพร่เชื้อจากสัตว์สู่มนุษย์ การศึกษาทางพันธุกรรมของไวรัสชี้ให้เห็นว่าบรรพบุรุษร่วมที่ใกล้ที่สุดของกลุ่ม HIV-1 M มีอายุย้อนไปถึงประมาณปี 1910 [ 267 ]ผู้สนับสนุนการกำหนดอายุนี้เชื่อมโยงการระบาดของ HIV กับการเกิดขึ้นของลัทธิล่าอาณานิคมและการเติบโตของเมืองอาณานิคมขนาดใหญ่ในแอฟริกา ซึ่งนำไปสู่การเปลี่ยนแปลงทางสังคม รวมถึงการมีเพศสัมพันธ์แบบไม่เลือกคู่มากขึ้น การแพร่กระจายของการค้าประเวณี และความถี่สูงของโรคแผลที่อวัยวะเพศ (เช่นโรคซิฟิลิส ) ในเมืองอาณานิคมที่เพิ่งก่อตั้งขึ้น[ 268 ]ในขณะที่อัตราการแพร่เชื้อ HIV ระหว่างการมีเพศสัมพันธ์ทางช่องคลอดนั้นต่ำภายใต้สถานการณ์ปกติ แต่จะเพิ่มขึ้นหลายเท่าหากคู่ใดคู่หนึ่งมีโรคติดต่อทางเพศสัมพันธ์ที่ทำให้เกิดแผลที่อวัยวะเพศ เมืองอาณานิคมในช่วงต้นทศวรรษ 1900 โดดเด่นในเรื่องอัตราการค้าประเวณีและแผลที่อวัยวะเพศที่สูงมาก โดยในปี 1928 เชื่อกันว่าผู้หญิงที่อาศัยอยู่ในคินชาซา ตะวันออกมากถึง 45% เป็นโสเภณี และในปี 1933 ประชากรประมาณ 15% ของเมืองเดียวกันนี้เป็นโรคซิฟิลิส[ 268 ]
มุมมองทางเลือกอีกประการหนึ่งคือ การปฏิบัติทางการแพทย์ที่ไม่ปลอดภัยในแอฟริกาหลังสงครามโลกครั้งที่สอง เช่น การนำเข็มฉีดยาแบบใช้ครั้งเดียวทิ้งกลับมาใช้ซ้ำโดยไม่ผ่านการฆ่าเชื้อในระหว่างการฉีดวัคซีนหมู่ การให้ยาปฏิชีวนะ และการรักษาด้วยยาต้านมาลาเรีย เป็นพาหะเริ่มต้นที่ทำให้ไวรัสสามารถปรับตัวเข้ากับมนุษย์และแพร่กระจายได้[ 265 ] [ 269 ] [ 270 ]
กรณีการติดเชื้อ HIV ในมนุษย์ที่ได้รับการบันทึกไว้อย่างดีครั้งแรกเกิดขึ้นในปี 1959 ในคองโก[ 271 ] ไวรัสอาจมีอยู่ในสหรัฐอเมริกาตั้งแต่ช่วงกลางถึงปลายทศวรรษ 1950 ชายอายุ 16 ปีชื่อโรเบิร์ต เรย์ฟอร์ดมีอาการในปี 1966 และเสียชีวิตในปี 1969 ในช่วงทศวรรษ 1970 มีกรณีที่ผู้คนติดเชื้อปรสิตและป่วยด้วยสิ่งที่เรียกว่า " โรคลำไส้เกย์ " แต่ปัจจุบันสงสัยว่าเป็นโรคเอดส์[ 272 ]
เชื่อกันว่ากรณีโรคเอดส์ที่ถูกอธิบายย้อนหลังครั้งแรกสุดนั้นเกิดขึ้นในนอร์เวย์ เริ่มต้นในปี 1966 โดยเป็นกรณีของArvid Noe [ 273 ] ในเดือนกรกฎาคม 1960 หลังจากคองโกได้รับเอกราชสหประชาชาติได้คัดเลือก ผู้เชี่ยวชาญและช่างเทคนิคที่พูด ภาษาฝรั่งเศสจากทั่วโลกเพื่อช่วยเติมเต็มช่องว่างด้านการบริหารที่เบลเยียม ทิ้งไว้ เนื่องจากเบลเยียมไม่ได้ทิ้งชนชั้นนำชาวแอฟริกันไว้บริหารประเทศ ในปี 1962 ชาวเฮติเป็นกลุ่มผู้เชี่ยวชาญที่มีการศึกษาดีเป็นอันดับสอง (จาก 48 กลุ่มชาติพันธุ์ที่ได้รับการคัดเลือก) ซึ่งมีจำนวนรวมประมาณ 4,500 คนในประเทศ[ 274 ] [ 275 ]ดร. Jacques Pépin ผู้เขียนชาวแคนาดาของหนังสือThe Origins of AIDSระบุว่าเฮติเป็นหนึ่งในจุดเริ่มต้นของเชื้อ HIV ในสหรัฐอเมริกา และชาวเฮติอาจนำเชื้อ HIV ข้ามมหาสมุทรแอตแลนติกกลับมาในช่วงทศวรรษ 1960 [ 275 ]แม้ว่าจะทราบกันว่ามีผู้ป่วยโรคเอดส์อย่างน้อยหนึ่งรายในสหรัฐอเมริกาตั้งแต่ปี 1966 [ 276 ]แต่การติดเชื้อส่วนใหญ่ที่เกิดขึ้นนอกแอฟริกาใต้ทะเลทรายซาฮารา (รวมถึงสหรัฐอเมริกา) สามารถสืบย้อนกลับไปถึงบุคคลที่ไม่ทราบชื่อเพียงคนเดียวที่ติดเชื้อเอชไอวีในเฮติและนำเชื้อมาสู่สหรัฐอเมริกาในช่วงประมาณปี 1969 [ 259 ]การระบาดแพร่กระจายอย่างรวดเร็วในกลุ่มเสี่ยงสูง (ในตอนแรกคือชายที่มีพฤติกรรมทางเพศกับชาย) ในปี 1978 อัตราการแพร่ระบาดของเชื้อเอชไอวี-1 ในกลุ่มชายรักร่วมเพศที่อาศัยอยู่ในนครนิวยอร์กและซานฟรานซิสโกอยู่ที่ประมาณ 5% ซึ่งบ่งชี้ว่ามีผู้ติดเชื้อหลายพันคนในประเทศ[ 259 ]
สังคมและวัฒนธรรม
ตราบาป

การตีตราผู้ติดเชื้อเอดส์มีอยู่ทั่วโลกในหลายรูปแบบ รวมถึงการกีดกันการปฏิเสธการเลือกปฏิบัติ และการหลีกเลี่ยงผู้ติดเชื้อเอชไอวี การตรวจหาเชื้อเอชไอวีโดยบังคับโดยไม่ได้รับความยินยอม ล่วงหน้าหรือ การรักษาความลับการใช้ความรุนแรงต่อผู้ติดเชื้อเอชไอวีหรือผู้ที่ถูกมองว่าติดเชื้อเอชไอวี และการกักกันผู้ติดเชื้อเอชไอวี[ 22 ]ความรุนแรงที่เกี่ยวข้องกับการตีตราหรือความกลัวความรุนแรงทำให้หลายคนไม่กล้าไปตรวจหาเชื้อเอชไอวี กลับไปรับผลตรวจ หรือเข้ารับการรักษา ซึ่งอาจเปลี่ยนโรคเรื้อรังที่สามารถจัดการได้ให้กลายเป็นโทษประหารชีวิตและทำให้เชื้อเอชไอวีแพร่กระจายต่อไป[ 278 ]
การตีตราผู้ป่วยเอดส์สามารถแบ่งออกเป็น 3 ประเภทดังต่อไปนี้:
- การตีตราโรคเอดส์แบบเครื่องมือ —การสะท้อนถึงความกลัวและความกังวลที่น่าจะเกี่ยวข้องกับโรคร้ายแรงและติดต่อได้[ 279 ]
- การตีตราเอดส์เชิงสัญลักษณ์ — การใช้ HIV/AIDS เพื่อแสดงทัศนคติต่อกลุ่มสังคมหรือวิถีชีวิตที่ถูกมองว่าเกี่ยวข้องกับโรค[ 279 ]
- การตีตราผู้ป่วยเอดส์ — การตีตราผู้ที่เกี่ยวข้องกับปัญหาเอชไอวี/เอดส์ หรือผู้ติดเชื้อเอชไอวี[ 280 ]
บ่อยครั้งที่การตีตราโรคเอดส์มักแสดงออกควบคู่ไปกับการตีตราอื่นๆ หนึ่งอย่างหรือมากกว่า โดยเฉพาะอย่างยิ่งการตีตราที่เกี่ยวข้องกับการรักร่วมเพศการรักสองเพศการมี เพศสัมพันธ์แบบไม่เลือกคู่ การค้าประเวณี และการใช้ยาเสพติดทางหลอดเลือดดำ[ 281 ]
ในประเทศที่พัฒนาแล้ว หลายแห่ง มีความสัมพันธ์ระหว่างโรคเอดส์กับพฤติกรรมรักร่วมเพศหรือรักสองเพศและความสัมพันธ์นี้มีความสัมพันธ์กับระดับอคติทางเพศที่สูงขึ้น เช่นทัศนคติต่อต้านรักร่วมเพศหรือต่อต้านรักสองเพศ[ 282 ]นอกจากนี้ยังมีการรับรู้ถึงความสัมพันธ์ระหว่างโรคเอดส์กับพฤติกรรมทางเพศระหว่างชายกับชายทั้งหมด รวมถึงการมีเพศสัมพันธ์ระหว่างชายที่ไม่ติดเชื้อ[ 279 ]อย่างไรก็ตาม รูปแบบการแพร่กระจายหลักของเชื้อเอชไอวีทั่วโลกยังคงเป็นการแพร่เชื้อทางเพศสัมพันธ์ระหว่างชายหญิง[ 283 ]
ผ้าห่มอนุสรณ์ผู้เสียชีวิตจากโรคเอดส์ ของโครงการ NAMESเกิดขึ้นในปี 1985 เพื่อเป็นการระลึกถึงชีวิตของผู้ที่เสียชีวิตจากโรคเอดส์ ในยุคที่ความอคติทางสังคมทำให้หลายคนไม่ได้รับการจัดงานศพ ปัจจุบันผ้าห่มนี้ได้รับการดูแลโดยอนุสรณ์สถานแห่งชาติเพื่อผู้เสียชีวิตจากโรคเอดส์ในซานฟรานซิสโก
ในปี พ.ศ. 2546 ซึ่งเป็นส่วนหนึ่งของการปฏิรูปกฎหมายการแต่งงานและประชากรโดยรวม ทำให้การแต่งงานของผู้ที่ได้รับการวินิจฉัยว่าเป็นโรคเอดส์กลายเป็นเรื่องถูกกฎหมายในประเทศจีน[ 284 ]
ระหว่างปี 2004 ถึง 2020 โซเมน เดบนัทได้เดินทางไปทั่วโลกด้วยจักรยานเพื่อส่งเสริมการรับรู้ เกี่ยว กับเอชไอวี / เอดส์
ในปี 2556 หอสมุดการแพทย์แห่งชาติสหรัฐอเมริกาได้พัฒนานิทรรศการเคลื่อนที่ชื่อSurviving and Thriving: AIDS, Politics, and Culture [ 285 ] ซึ่งครอบคลุมถึงงานวิจัยทางการแพทย์ การตอบสนองของรัฐบาลสหรัฐฯ และเรื่องราวส่วนตัวจากผู้ป่วยโรคเอดส์ ผู้ดูแล และนักเคลื่อนไหว[ 286 ]
อคติได้พิสูจน์แล้วว่าเป็นอุปสรรคต่อการปรับปรุงPrEPภายในชุมชน MSM อุปสรรคที่ใหญ่ที่สุดในการใช้ PrEP คืออคติเกี่ยวกับ HIV และชายรักร่วมเพศ ชายรักร่วมเพศที่ใช้ PrEP ประสบกับ " การดูถูกเหยียดหยามทางเพศ " [ 287 ] [ 288 ] มีการระบุอุปสรรคอื่นๆ อีกมากมาย รวมถึงการขาดการดูแล LGBTQ ที่มีคุณภาพ ค่าใช้จ่าย และการปฏิบัติตามการใช้ยา[ 289 ]
ผลกระทบทางเศรษฐกิจ

โรคเอดส์ส่งผลกระทบต่อเศรษฐกิจของทั้งบุคคลและประเทศ[ 290 ]ผลิตภัณฑ์มวลรวมภายในประเทศของประเทศที่ได้รับผลกระทบมากที่สุดลดลงเนื่องจากการขาดแคลนทุนมนุษย์[ 290 ] [ 291 ]หากขาดโภชนาการ การดูแลสุขภาพ และยาที่เหมาะสม ผู้คนจำนวนมากจะเสียชีวิตจากภาวะแทรกซ้อนที่เกี่ยวข้องกับโรคเอดส์ ก่อนเสียชีวิต พวกเขาจะไม่เพียงแต่ไม่สามารถทำงานได้ แต่ยังต้องการการดูแลทางการแพทย์อย่างมาก มีการประมาณการว่าในปี 2550 มีเด็กกำพร้าจากโรคเอดส์ 12 ล้าน คน[ 290 ]หลายคนได้รับการดูแลจากปู่ย่าตายายผู้สูงอายุ[ 292 ]
การกลับไปทำงานหลังจากเริ่มการรักษาเอชไอวี/เอดส์เป็นเรื่องยาก และผู้ที่ได้รับผลกระทบมักทำงานน้อยกว่าคนทำงานทั่วไปการว่างงานในผู้ติดเชื้อเอชไอวี/เอดส์ยังเกี่ยวข้องกับความคิดฆ่าตัวตายปัญหาความจำ และการแยกตัวทางสังคม การมีงานทำช่วยเพิ่มความภาคภูมิใจในตนเองความรู้สึกมีศักดิ์ศรี ความมั่นใจ และคุณภาพชีวิตของผู้ติดเชื้อเอชไอวี/เอดส์ การรักษาด้วยยาต้านไวรัสอาจช่วยให้ผู้ติดเชื้อเอชไอวี/เอดส์ทำงานได้มากขึ้น และอาจเพิ่มโอกาสที่ผู้ติดเชื้อเอชไอวี/เอดส์จะได้งานทำ (หลักฐานคุณภาพต่ำ) [ 293 ]
โรคเอดส์ซึ่งส่วนใหญ่ส่งผลกระทบต่อคนหนุ่มสาว ทำให้จำนวนประชากรที่ต้องเสียภาษีลดลง ส่งผลให้ทรัพยากรที่มีอยู่สำหรับการใช้จ่ายสาธารณะเช่น การศึกษาและบริการด้านสุขภาพที่ไม่เกี่ยวข้องกับโรคเอดส์ลดลง ส่งผลให้งบประมาณของรัฐมีแรงกดดันมากขึ้น และเศรษฐกิจเติบโตช้าลง สิ่งนี้ทำให้ฐานภาษีเติบโตช้าลง ซึ่งผลกระทบนี้จะยิ่งรุนแรงขึ้นหากมีค่าใช้จ่ายเพิ่มขึ้นในการรักษาผู้ป่วย การฝึกอบรม (เพื่อทดแทนคนงานที่ป่วย) ค่าจ้างในระหว่างลาป่วย และการดูแลเด็กกำพร้าจากโรคเอดส์ โดยเฉพาะอย่างยิ่งหากอัตราการเสียชีวิตของผู้ใหญ่ที่เพิ่มขึ้นอย่างรวดเร็วทำให้ภาระในการดูแลเด็กกำพร้าเหล่านี้เปลี่ยนจากครอบครัวไปเป็นรัฐบาล[ 292 ]
ในระดับครัวเรือน โรคเอดส์ทำให้เกิดการสูญเสียรายได้และค่าใช้จ่ายด้านการดูแลสุขภาพที่เพิ่มขึ้น การศึกษาในประเทศโกตดิวัวร์แสดงให้เห็นว่าครัวเรือนที่มีผู้ติดเชื้อเอชไอวี/เอดส์ใช้จ่ายด้านการแพทย์มากกว่าครัวเรือนอื่นๆ ถึงสองเท่า ค่าใช้จ่ายเพิ่มเติมนี้ยังทำให้มีรายได้เหลือน้อยลงสำหรับการใช้จ่ายด้านการศึกษาและการลงทุนส่วนตัวหรือครอบครัวอื่นๆ[ 294 ]
ศาสนาและเอดส์
หัวข้อเรื่องศาสนาและเอดส์กลายเป็นประเด็นถกเถียงอย่างมาก โดยเฉพาะอย่างยิ่งเพราะผู้นำทางศาสนาบางกลุ่มได้ประกาศต่อต้านการใช้ถุงยางอนามัยอย่างเปิดเผย[ 295 ] [ 296 ]แนวทางทางศาสนาในการป้องกันการแพร่กระจายของเอดส์ ตามรายงานของแมทธิว แฮนลีย์ ผู้เชี่ยวชาญด้านสุขภาพชาวอเมริกัน เรื่อง " คริสตจักรคาทอลิกและวิกฤตเอดส์โลก"ระบุว่าจำเป็นต้องมีการเปลี่ยนแปลงทางวัฒนธรรม รวมถึงการเน้นย้ำเรื่องความซื่อสัตย์ในชีวิตสมรสและการงดเว้นการมีเพศสัมพันธ์นอกสมรส[ 296 ]
องค์กรทางศาสนาบางแห่งอ้างว่าการอธิษฐานสามารถรักษาโรคเอดส์ได้ ในปี 2554 บีบีซีรายงานว่าโบสถ์บางแห่งในลอนดอนอ้างว่าการอธิษฐานจะรักษาโรคเอดส์ได้ และ ศูนย์ศึกษาด้านสุขภาพทางเพศและเอชไอวี ในแฮกนีย์รายงานว่ามีหลายคนหยุดรับประทานยา บางครั้งตามคำแนะนำโดยตรงของบาทหลวง ซึ่งนำไปสู่การเสียชีวิตจำนวนมาก[ 297 ]โบสถ์Synagogue Church Of All Nationsโฆษณา "น้ำเจิม" เพื่อส่งเสริมการรักษาของพระเจ้า แม้ว่ากลุ่มดังกล่าวจะปฏิเสธว่าไม่ได้แนะนำให้ผู้คนหยุดรับประทานยา[ 297 ]
การนำเสนอของสื่อ
หนึ่งในกรณีแรกๆ ที่มีชื่อเสียงของโรคเอดส์คือร็อก ฮัดสัน นักแสดงเกย์ชาวอเมริกัน เขาได้รับการวินิจฉัยในปี 1984 ประกาศว่าตนเองติดเชื้อไวรัสเมื่อวันที่ 25 กรกฎาคม 1985 และเสียชีวิตในอีกไม่กี่เดือนต่อมาในวันที่ 2 ตุลาคม 1985 [ 298 ]อีกหนึ่งผู้เสียชีวิตจากโรคเอดส์ชาวอังกฤษที่โดดเด่นในปีนั้นคือนิโคลัส อีเดนนักการเมืองเกย์และบุตรชายของอดีตนายกรัฐมนตรีแอนโทนี อีเดน [ 299 ] เมื่อวันที่ 24 พฤศจิกายน 1991 เฟรดดี เมอร์คิวรี นักดนตรีร็อคชาวอังกฤษ เสียชีวิตจากโรคที่เกี่ยวข้องกับเอดส์ หลังจากเปิดเผยการวินิจฉัยโรคเพียงวันก่อนหน้า[ 300 ]
หนึ่งในกรณีการติดเชื้อไวรัสในกลุ่มคนรักต่างเพศที่มีชื่อเสียงเป็นครั้งแรกคืออาร์เธอร์ แอช นักเทนนิสชาวอเมริกัน เขาได้รับการวินิจฉัยว่าติดเชื้อเอชไอวีเมื่อวันที่ 31 สิงหาคม พ.ศ. 2531 โดยติดเชื้อจากการรับเลือดระหว่างการผ่าตัดหัวใจในช่วงต้นทศวรรษ พ.ศ. 2523 การตรวจเพิ่มเติมภายใน 24 ชั่วโมงหลังจากการวินิจฉัยครั้งแรกพบว่าแอชเป็นโรคเอดส์ แต่เขาไม่ได้เปิดเผยการวินิจฉัยของเขาต่อสาธารณชนจนกระทั่งเดือนเมษายน พ.ศ. 2535 [ 301 ]เขาเสียชีวิตจากโรคนี้เมื่อวันที่ 6 กุมภาพันธ์ พ.ศ. 2536 ขณะอายุ 49 ปี[ 302 ]
ภาพถ่ายของ Therese Frare ที่ถ่ายDavid Kirby นักเคลื่อนไหวเพื่อสิทธิเกย์ ขณะที่เขากำลังจะเสียชีวิตจากโรคเอดส์โดยมีครอบครัวอยู่รอบข้าง ถ่ายเมื่อเดือนเมษายน พ.ศ. 2533 นิตยสาร Lifeกล่าวว่าภาพนี้กลายเป็นภาพที่ "มีความเชื่อมโยงอย่างทรงพลังที่สุดกับการระบาดของเชื้อ HIV/AIDS" ภาพนี้ถูกนำเสนอในนิตยสาร Lifeได้รับรางวัลWorld Press Photoและโด่งดังไปทั่วโลกหลังจากถูกนำไปใช้ในแคมเปญโฆษณาของ United Colors of Benetton ในปี พ.ศ. 2535 [ 303 ]
ศิลปินชื่อดังและนักเคลื่อนไหวต่อต้านเอดส์หลายคน เช่นLarry Kramer , Diamanda GalásและRosa von Praunheim [ 304 ]รณรงค์เรื่องการศึกษาเกี่ยวกับเอดส์และสิทธิของผู้ที่ได้รับผลกระทบ ศิลปินเหล่านี้ทำงานโดยใช้สื่อหลากหลายรูปแบบ
การส่งต่ออาชญากรรม
การแพร่เชื้อเอชไอวี โดยเจตนาหรือโดยประมาท คือ การติดเชื้อ ไวรัสภูมิคุ้มกันบกพร่อง ในมนุษย์ (HIV) ให้แก่บุคคลอื่นบางประเทศหรือเขตอำนาจศาล รวมถึงบางพื้นที่ของสหรัฐอเมริกา มีกฎหมายที่กำหนดให้การแพร่เชื้อหรือการสัมผัสเชื้อเอชไอวีเป็นความผิดทางอาญา[ 305 ]บางประเทศอาจตั้งข้อหาผู้ถูกกล่าวหาภายใต้กฎหมายที่ตราขึ้นก่อนการระบาดของเอชไอวี
ในปี 1996 จอห์นสัน อาซิกาชาวแคนาดาที่เกิดในอูกันดาได้รับการวินิจฉัยว่าติดเชื้อเอชไอวี ต่อมาเขามีเพศสัมพันธ์โดยไม่ป้องกันกับผู้หญิง 11 คนโดยไม่เปิดเผยการวินิจฉัยโรคของเขา ภายในปี 2003 มีผู้หญิง 7 คนติดเชื้อเอชไอวี และ 2 คนเสียชีวิตจากภาวะแทรกซ้อนที่เกี่ยวข้องกับโรคเอดส์[ 306 ] [ 307 ]อาซิกาถูกตัดสินว่ามีความผิด ฐาน ฆาตกรรมระดับหนึ่งและถูกตัดสิน จำคุก ตลอดชีวิต[ 308 ]
ความเข้าใจผิด
มีความเข้าใจผิดมากมายเกี่ยวกับเชื้อ HIV และโรคเอดส์ความเข้าใจผิดสามประการคือ โรคเอดส์สามารถแพร่กระจายได้จากการสัมผัสแบบไม่ตั้งใจการมีเพศสัมพันธ์กับหญิงพรหมจรรย์จะรักษาโรคเอดส์ได้[ 309 ] [ 310 ] [ 311 ]และเชื้อ HIV สามารถติดเชื้อได้เฉพาะในกลุ่มชายรักร่วมเพศและผู้ใช้ยาเสพติดเท่านั้น[ 312 ] [ 313 ]ในปี 2014 ประชาชนชาวอังกฤษบางส่วนเข้าใจผิดว่าสามารถติดเชื้อ HIV ได้จากการจูบ (16%) การใช้แก้วร่วมกัน (5%) การถ่มน้ำลาย (16%) การใช้ที่นั่งชักโครกสาธารณะ (4%) และการไอหรือจาม (5%) [ 314 ]ความเข้าใจผิดอื่นๆ คือ การมีเพศสัมพันธ์ทางทวารหนักระหว่างชายรักร่วมเพศสองคนที่ไม่ได้ติดเชื้อสามารถนำไปสู่การติดเชื้อ HIV ได้ และการพูดคุยอย่างเปิดเผยเกี่ยวกับ HIV และรักร่วมเพศในโรงเรียนจะนำไปสู่การเพิ่มขึ้นของอัตราการติดเชื้อเอดส์[ 315 ]
กลุ่มคนจำนวนน้อยยังคงโต้แย้งถึงความเชื่อมโยงระหว่างเชื้อ HIV และโรคเอดส์[ 316 ]การมีอยู่ของเชื้อ HIV เอง หรือความถูกต้องของการทดสอบและวิธีการรักษาเชื้อ HIV [ 317 ] [ 318 ]ข้อกล่าวอ้างเหล่านี้ ซึ่งรู้จักกันในชื่อการปฏิเสธโรคเอดส์ได้รับการตรวจสอบและปฏิเสธโดยชุมชนวิทยาศาสตร์[ 319 ]อย่างไรก็ตาม ข้อกล่าวอ้างเหล่านี้มีผลกระทบทางการเมืองอย่างมาก โดยเฉพาะในแอฟริกาใต้ซึ่งการที่รัฐบาลยอมรับการปฏิเสธโรคเอดส์อย่างเป็นทางการ (ค.ศ. 1999–2005) เป็นสาเหตุให้การรับมือกับการระบาดของโรคเอดส์ในประเทศนั้นไม่มีประสิทธิภาพ และถูกกล่าวหาว่าเป็นสาเหตุของการเสียชีวิตและการติดเชื้อ HIV ที่สามารถหลีกเลี่ยงได้หลายแสนราย[ 320 ] [ 321 ] [ 322 ]
ทฤษฎีสมคบคิดที่ถูกหักล้างไปแล้วหลาย ทฤษฎี ระบุว่าเชื้อ HIV ถูกสร้างขึ้นโดยนักวิทยาศาสตร์ ไม่ว่าจะโดยไม่ได้ตั้งใจหรือโดยเจตนาปฏิบัติการ INFEKTIONเป็น ปฏิบัติการ เชิงรุก ของโซเวียตทั่วโลก เพื่อเผยแพร่ข้อกล่าวอ้างที่ว่าสหรัฐอเมริกาเป็นผู้สร้างเชื้อ HIV/AIDS ผลสำรวจแสดงให้เห็นว่ามีผู้คนจำนวนมากที่เชื่อ—และยังคงเชื่อ—ในข้อกล่าวอ้างดังกล่าว[ 323 ]
วิจัย
การวิจัยเกี่ยวกับเอชไอวี/เอดส์ ครอบคลุมถึงการวิจัยทางการแพทย์ ทั้งหมด ที่พยายามป้องกัน รักษา หรือบำบัดเอชไอวี/เอดส์ ตลอดจนการวิจัยพื้นฐานเกี่ยวกับธรรมชาติของเชื้อเอชไอวีในฐานะตัวก่อโรค และเกี่ยวกับเอดส์ในฐานะโรคที่เกิดจากเชื้อเอชไอวี
รัฐบาลและสถาบันวิจัยหลายแห่งมีส่วนร่วมในการวิจัยเกี่ยวกับเอชไอวี/เอดส์ การวิจัยนี้รวมถึงการแทรกแซงด้านสุขภาพ เชิงพฤติกรรม เช่นการศึกษาเรื่องเพศและการพัฒนายาเช่น การวิจัยเกี่ยวกับสารฆ่าเชื้อจุลินทรีย์สำหรับโรคติดต่อทางเพศสัมพันธ์วัคซีนเอชไอวีและยาต้านไวรัสเอชไอวีพื้นที่การวิจัยทางการแพทย์อื่นๆ ได้แก่ หัวข้อการป้องกันก่อนการสัมผัสเชื้อการป้องกันหลังการสัมผัสเชื้อและ การขลิบ และการติดเชื้อเอชไอวีเจ้าหน้าที่สาธารณสุข นักวิจัย และโครงการต่างๆ สามารถได้รับภาพรวมที่ครอบคลุมมากขึ้นเกี่ยวกับอุปสรรคที่พวกเขาเผชิญ และประสิทธิภาพของแนวทางปัจจุบันในการรักษาและป้องกันเอชไอวี โดยการติดตามตัวชี้วัดเอชไอวีมาตรฐาน[ 324 ]การใช้ตัวชี้วัดทั่วไปเป็นจุดสนใจที่เพิ่มขึ้นขององค์กรพัฒนาและนักวิจัย[ 325 ] [ 326 ]
External links
- UNAIDS – Joint United Nations Program on HIV/AIDS
- HIVinfo – Information on HIV/AIDS treatment, prevention, and research, U.S. Department of Health and Human Services
- 2018 Recommendations of the International Antiviral Society
สรุปเนื้อหา
ข้อมูลสำคัญจากบทความ
ข้อมูลสำคัญเกี่ยวกับ HIV/AIDS
The human immunodeficiency virus (HIV) is a retrovirus that attacks the immune system.
Signs and symptoms
There are three main stages of HIV infection: acute infection, clinical latency, and AIDS. [ 1 ] [ 29 ]
First main stage: acute infection
The initial period following infection with HIV is called acute HIV, primary HIV or acute retroviral syndrome.
Second main stage: clinical latency
The initial symptoms are followed by a stage called clinical latency, asymptomatic HIV, or chronic HIV.